True teeth cannot grow just anywhere on your body. Tooth development is a highly specific biological process that requires a precise combination of tissue types, molecular signals, and structural organization that only exists in the jaw during development. What people sometimes find in unusual places, like a hard bump in the nose, a firm nodule under the skin, or a lump in the gum behind a normal tooth, is almost never a "new tooth" in the full biological sense. It is usually an ectopic (misplaced) tooth that was already developing, a tooth-like calcified lesion, or an odontogenic tumor. The distinction matters a lot because the cause, risk level, and treatment are completely different depending on what it actually is.
Can Teeth Grow in Other Parts of the Body? What’s Real

Marcus Holloway
27 Apr 2026

Where tooth-like structures actually show up (and what they really are)

People occasionally discover hard, calcified lumps in places that have nothing to do with their normal teeth. The most documented non-oral location is the nasal cavity. There are genuine published case reports of teeth erupting into the nose, usually from a supernumerary (extra) tooth or a misplaced permanent tooth that migrated upward during development rather than erupting normally through the gum.
These intranasal teeth cause symptoms like nasal obstruction, unexplained nosebleeds, or chronic rhinitis, and they are removed surgically, often endoscopically. A systematic review describes endoscopic removal of ectopic sinonasal teeth as a common management approach when they are identified or cause symptoms [ectopic sinonasal teeth are removed surgically, often endoscopically](https://link. springer. com/article/10.
1186/s40463-019-0353-8). CT imaging is the key diagnostic tool here because a true ectopic tooth will show the characteristic density of mineralized tissue along with a central pulp cavity, which distinguishes it from a foreign body or a calcium deposit called a rhinolith.
Other "tooth-like" findings people stumble across include odontomas, calcifying odontogenic cysts, and osteoma cutis. An odontoma is a benign lesion made of disorganized enamel, dentin, and cementum-like material. It can look like a small calcified mass on an X-ray and occasionally erupts through soft tissue, but it is not an organized tooth with a crown, root, and pulp laid out the way a real tooth is.
A calcifying odontogenic cyst produces ghost cells and calcium deposits from odontogenic epithelium, which can fool even experienced clinicians on imaging until a biopsy is done. Osteoma cutis is bone formation in the skin or soft tissue, completely unrelated to the dental development pathway, but it produces firm, calcified nodules that some people worry are tooth-related. None of these are teeth in the true developmental sense.
The bottom line: when something tooth-like shows up in an unusual location, it is almost always one of three things. Either it is a real tooth that was already forming but erupted somewhere it should not have (ectopic eruption), a disorganized mass of tooth-tissue components (like an odontoma), or a calcification that has nothing to do with the odontogenic pathway at all. A brand-new tooth spontaneously forming in your finger, your skin, or your stomach is not how human biology works.
Why teeth are essentially locked to the jaw
Tooth development, called odontogenesis, is one of the most tightly regulated processes in human biology. It requires a back-and-forth chemical conversation between two very specific tissue types: oral ectoderm-derived epithelium and neural crest-derived ectomesenchyme. This signaling involves multiple molecular pathways, including WNT/beta-catenin, BMP, FGF, SHH (the Hedgehog pathway), and EDA. These pathways have to fire in the right sequence, in the right tissue context, at the right developmental window, to produce the structures (the enamel organ, the dental papilla, the tooth germ) that eventually become a tooth. If the WNT signaling is disrupted, for example, tooth development arrests at the bud stage. These are not conditions that arise spontaneously in adult soft tissue.
For enamel and dentin to actually form, you need ameloblasts and odontoblasts, specialized cells that only differentiate in the context of the epithelial-mesenchymal junction of a developing tooth germ. Ameloblasts secrete enamel; odontoblasts secrete dentin. Outside of a true odontogenic development context, these cells simply do not appear. This is also why enamel cannot regenerate after it is lost: ameloblasts disappear once enamel formation is complete. They regress and undergo apoptosis, leaving no cell population behind that could rebuild enamel if it wears away or gets damaged. This is a hard biological limit, not a gap in current dental technology.
The jaw is uniquely set up for tooth formation during development because that is where the dental lamina forms, where tooth germs are organized, and where the alveolar bone builds up to house and support erupting teeth. No other region of the body goes through that specific developmental program, which is exactly why teeth do not randomly appear on fingers, in ears, or on skin, despite what some alarming internet posts might suggest.
The real exceptions: impacted teeth, supernumerary teeth, and wisdom teeth

The cases that confuse people most are ones where a tooth shows up in a place they did not expect, but still within the broader jaw and skull region. These are not random new teeth forming from scratch. They are teeth that were always part of the developmental program but went wrong somewhere along the way.
Supernumerary teeth
Supernumerary teeth are extra teeth, meaning teeth beyond the normal complement of 20 baby teeth or 32 adult teeth. They form because the dental lamina produces an extra tooth germ, and they can appear almost anywhere in the dental arch. The most common type is the mesiodens, a small extra tooth that forms between the upper front teeth and can block the normal incisors from erupting properly. Supernumeraries can also migrate into the nasal floor, the palate, or other nearby anatomical spaces before or after eruption. These are the most common explanation for "teeth in unusual places" within the head and neck region.
Impacted teeth
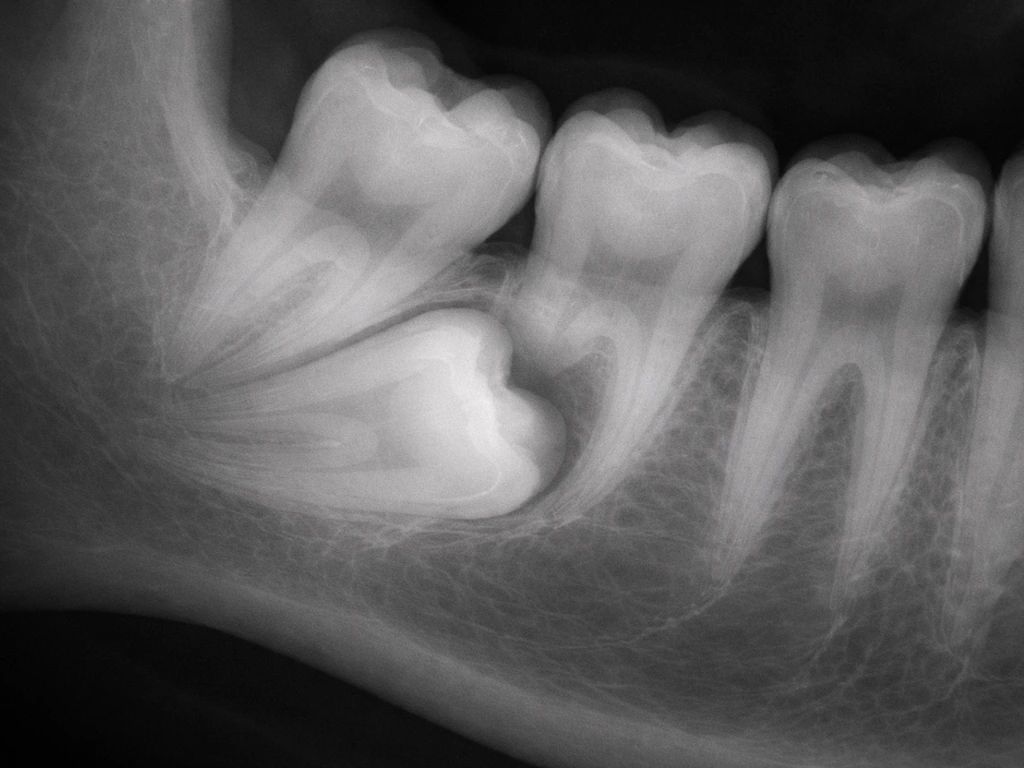
An impacted tooth is one that fails to erupt fully because it is blocked by another tooth, bone, or soft tissue. Impacted teeth are not growing somewhere new; they are stuck where they formed and either stay buried or, occasionally, find an abnormal path to the surface. Impacted canines, for example, can sometimes erupt through the roof of the mouth rather than through the normal gum position. Syndromes like cleidocranial dysplasia (caused by mutations in the RUNX2 gene) are associated with large numbers of impacted and supernumerary teeth, sometimes dozens of them visible on panoramic X-rays.
Wisdom teeth
Wisdom teeth are the third molars, the last teeth to develop and erupt, usually between ages 17 and 25. They are a normal part of human tooth development, not an anomaly, but they become problematic when there is not enough jaw space for them to come in correctly. They may stay partially or fully impacted, erupt at an angle, or create pressure against neighboring teeth. When someone feels a new bump or pressure at the back of their jaw in their late teens or early twenties, it is almost always a wisdom tooth and not some mysterious new dental growth.
What to do if you find a tooth-like bump in an unusual place

If you or your child notices a hard lump, bump, or what feels like a tooth erupting somewhere it should not be, do not panic, but do not ignore it either. The range of possibilities is wide (from completely benign to something that needs prompt treatment), and imaging is almost always needed to figure out what you are dealing with.
- Start with a dentist or oral surgeon if the bump is anywhere near the jaw, gum, palate, or floor of the mouth. They can order a periapical X-ray or a panoramic radiograph as a first step to see if there is an odontogenic structure involved.
- See an ENT (ear, nose, and throat specialist) if the issue is in or near the nose, sinuses, or throat. Intranasal teeth are managed by ENT surgeons, often with endoscopic removal.
- Go to a dermatologist if the lesion is in the skin or soft tissue of the face, neck, or body and is not associated with the jaw. Osteoma cutis and foreign body granulomas fall into this category.
- Ask for a CT scan. For any tooth-like radiopaque lesion in an unusual location, a CT gives you three-dimensional information about the size, shape, position, and internal structure of the lesion. A true ectopic tooth will have a central pulp cavity on CT; a rhinolith or foreign body will not.
- Request a biopsy if imaging is inconclusive or if the lesion has features that concern your provider. Odontogenic cysts, calcifying odontogenic cysts, and ghost cell tumors are diagnosed histologically, not just by imaging.
Good questions to ask your provider include: Is this a true tooth or a calcified lesion? Is there any sign of an underlying syndrome like cleidocranial dysplasia or Gardner syndrome, which can cause multiple extra or misplaced teeth? Does this need to come out now, or can we watch it? What is the risk to adjacent structures if we leave it?
Gardner syndrome is worth mentioning here because it is an autosomal dominant condition associated with supernumerary teeth, odontomas, osteomas, and colorectal polyps. If a patient has multiple unusual dental findings alongside jaw osteomas or soft-tissue masses, a genetics referral is appropriate. Similarly, if a child has a panoramic X-ray showing an unusual number of impacted or extra teeth, cleidocranial dysplasia should be on the list to rule out.
Can teeth, gums, or enamel actually grow back after damage?
This is one of the most common misconceptions in dental health, and the answer depends entirely on what you are asking about. Enamel, dentin, cementum, and the periodontal ligament all behave very differently when it comes to regeneration.
| Structure | Can it regenerate? | What actually happens | Current clinical options |
|---|---|---|---|
| Enamel | No | Ameloblasts disappear after tooth formation; no cells remain to rebuild enamel | Remineralization (fluoride, casein phosphopeptide) can repair early lesions; lab research on biomimetic enamel is ongoing |
| Dentin | Partially | Odontoblasts remain in the pulp and can form reparative/secondary dentin in response to injury | Pulp capping with bioactive materials (MTA, biodentine) can stimulate dentin bridge formation; clinical trials show success with growth factors like rhPDGF |
| Cementum | Partially | Cementoblasts retain some regenerative capacity, relevant in periodontal therapy | Periodontal regeneration procedures (grafts, membranes, growth factors) can restore cementum and bone support |
| Periodontal ligament | Partially | Has mesenchymal stem cell populations that contribute to repair | Guided tissue regeneration and growth factor therapies support PDL repair |
| Whole tooth | No (in humans) | Humans are diphyodonts (two sets only); no third dentition forms naturally | Implants, bridges, and dentures replace lost teeth; lab research on biological tooth regeneration is early-stage |
The most practical takeaway here is that dentin can genuinely respond to injury and form a protective bridge, especially when a dentist uses a bioactive pulp capping material. A randomized clinical trial has demonstrated that recombinant human platelet-derived growth factor combined with MTA for pulp capping can stimulate secondary dentin regeneration. That is real regeneration, but it is happening inside an existing tooth in a controlled clinical setting, not spontaneous regrowth of a lost tooth. Enamel remineralization with fluoride or other mineralization-promoting agents can reverse early-stage white spot lesions and slow decay, but it cannot rebuild a cavity or a chip. The structure is not regenerated; surface mineral density is improved.
Gum tissue (gingiva) can heal and reattach to some extent after injury or surgery, but significant gum recession does not spontaneously reverse. Gum grafts are the standard treatment when recession has progressed past a certain point. The popular idea that gums can "grow back" on their own with better brushing is a myth worth busting: you can stop further recession by improving oral hygiene, but you cannot undo what is already lost without intervention.
Risk factors and prevention for abnormal tooth development
Most cases of supernumerary teeth, ectopic eruption, and other abnormal tooth development are not preventable in the traditional sense, because they are rooted in genetics and developmental timing rather than lifestyle choices. But understanding the risk factors helps you know when to be proactive about screening and monitoring.
- Family history of supernumerary teeth: extra teeth tend to run in families, so if a parent or sibling had them, early panoramic X-rays in children (around age 7 to 8) are a good idea
- Known genetic syndromes: cleidocranial dysplasia (RUNX2 mutations), Gardner syndrome (APC gene mutations), and Down syndrome are all associated with higher rates of abnormal tooth development, including supernumeraries and impacted teeth
- History of trauma to the face or jaw in childhood: trauma can displace developing tooth buds and contribute to ectopic eruption patterns, as seen in some cases of intranasal teeth following facial injury
- Cleft palate: children with cleft lip and palate have higher rates of missing, malformed, or ectopically positioned teeth in the cleft region
- Crowding and delayed eruption: if a child's baby teeth are not falling out on the expected schedule or a permanent tooth seems to be taking an unusual path, early dental evaluation can catch ectopic eruption before it causes significant problems
- Radiation to the head and neck during childhood: can disrupt tooth development and increase the risk of developmental anomalies in teeth that were forming at the time of treatment
The single most useful preventive step for catching abnormal tooth development early is a panoramic radiograph around age 7 to 8, which most pediatric dentists recommend anyway as part of orthodontic screening. This one image can reveal supernumerary teeth, impacted teeth, odontomas, and cysts before they cause symptoms or damage neighboring teeth. If you are an adult who has never had a full-mouth X-ray series and you have noticed odd dental history (teeth that never came in, asymmetric eruption, unexplained swelling), it is worth asking your dentist about getting one now.
The broader point is this: teeth do not randomly sprout in new locations as you age. What looks like a tooth in an unusual place is almost always something that has been there since development, either waiting to erupt, sitting impacted, or slowly growing as an odontogenic lesion. In other words, what people describe as teeth that grow on top of teeth are usually supernumerary teeth or other odontogenic growths rather than true tooth-to-tooth growth. Catching these things early, before they cause obstruction, infection, or damage to adjacent teeth, is the whole game. When in doubt, see a dentist, get the imaging, and ask the specific questions that get you a real answer.
FAQ
If I have a hard bump under the skin or in my nose, how can I tell if it is a true ectopic tooth versus a calcified lesion?
You generally cannot tell reliably by touch or appearance. Clinicians use imaging to look for mineralized tissue patterns that resemble tooth structure, and they may use CT for location and density. A key differentiator is whether there is a tooth-like organization that suggests a developing tooth, versus a lesion that is mostly calcification. If imaging is unclear, a biopsy is often what definitively separates a tooth from odontogenic tumors or cysts.
Can a tooth that is already in my jaw slowly migrate upward or change position over time?
Yes, migration can happen in certain situations, especially with supernumerary teeth or teeth that are positioned abnormally from the start. They may drift into nearby spaces as growth and eruption occur, which can make the finding seem like it is “appearing” later. However, new tooth formation in an unrelated adult tissue is not the usual explanation.
Could a dental infection cause a new tooth to form in an unusual location?
Typically no. Infections usually cause pain, swelling, bone changes, and cystic or inflammatory lesions, but they do not restart the developmental process needed to build a new tooth in soft tissue. A painful lump in an odd area still warrants evaluation because it could be an odontogenic tumor, a cyst, or another cause that needs different treatment.
If a child has a supernumerary tooth, should other family members be screened?
Often, yes. Because some conditions associated with multiple extra teeth have genetic links, discussing family history with the dentist or pediatrician is important. Your provider may recommend earlier panoramic imaging for relatives if there is a pattern of unusual dental findings or related systemic features.
When is it better to monitor versus remove an ectopic or impacted tooth?
It depends on symptoms and risk to neighboring structures. If the tooth is asymptomatic and not threatening adjacent teeth, nerves, or sinuses, clinicians may choose periodic monitoring with repeat imaging. If it is causing obstruction, recurrent infections, damage to adjacent roots, or significant displacement, removal or treatment is more likely. The decision is usually individualized based on imaging findings and proximity to critical anatomy.
Do enamel or dentin regrow if I remove a “tooth-like” mass that is not a true tooth?
Usually not in the way people expect. If the finding is an odontoma, cyst, or another calcified lesion, the tissue is not comparable to a normal tooth germ, so removing it does not trigger the body to regenerate organized enamel, dentin, and pulp. Treatment focuses on removal or management of the lesion, plus follow-up imaging to ensure it does not recur or cause complications.
Can fluoride or other remineralization treatments make something like an ectopic tooth or odontogenic lesion disappear?
No. Fluoride and remineralization therapies help with early enamel demineralization (white spot lesions) and slow decay, but they do not dissolve a tooth-like calcified lesion or stop odontogenic tumor or cyst biology. If imaging suggests an odontogenic cause, the pathway is typically dental or surgical management rather than cavity-care products.
Are panoramic X-rays enough to diagnose an ectopic tooth in the nose or other unusual sites?
A panoramic film can be a good starting screen for abnormal teeth in the jaws, but CT is often the key test for suspected intranasal teeth or complicated calcified findings. CT helps confirm exact location, density, and whether there is tooth-like internal structure. Your clinician will choose imaging based on symptoms and where the finding is located.
What symptoms should prompt urgent evaluation rather than waiting for a routine dental visit?
Seek prompt care if there is difficulty breathing through the nose, frequent or heavy nosebleeds, rapidly enlarging swelling, fever with facial pain, worsening drainage, numbness, or signs of spreading infection. For mouth or jaw findings, urgency increases if there is severe pain, pus, trouble swallowing, or accelerated swelling.
Could “teeth growing on top of teeth” actually be something other than supernumerary teeth?
Yes. Similar appearances can come from odontomas, calcifying odontogenic cysts, or other calcified odontogenic lesions. Imaging plus an assessment of symptoms and location usually determines whether the finding is truly an extra tooth, an odontogenic mass, or a non-tooth calcification.
Next Articles

Do Milk Teeth Grow Back? Timelines, What to Do, Red Flags
Learn if milk teeth regrow, typical timelines for permanent teeth, what to do after loss or injury, and red flags.

Can Milk Teeth Grow Twice? Replacement vs True Regrowth
Can milk teeth grow twice? Learn why baby teeth usually only get replaced, not regrown, and what to do if one falls out

Why Do Teeth Only Grow Twice? Baby vs Permanent Explained
Why humans have only baby and permanent teeth: eruption timeline, limits of enamel regrowth, and common exceptions to kn