Yes, wisdom teeth can absolutely grow in during your 20s. The typical eruption window runs from about 17 to 25, which means your mid-to-late 20s are still completely within normal territory. Some people feel them pushing through at 18; others don't notice anything until 23 or 24. If you're in your 20s and suddenly feeling pressure, soreness, or swelling at the back of your mouth, there's a real chance a third molar is on the move.
Can Wisdom Teeth Grow in Your 20s? Signs and Next Steps

Marcus Holloway
27 Apr 2026

Wisdom tooth eruption timeline: what's normal into your 20s

The American Dental Association puts the classic eruption window at ages 17 to 21, while the American Association of Oral and Maxillofacial Surgeons extends that range to 17 to 25. Both are right in different ways: the average person starts noticing movement in the late teens, but eruption can drag on for years. One tooth might partially emerge at 19, and the one next to it might not budge until 23. That's not unusual, that's just how variable third molar development is.
Research using panoramic X-rays has shown that the minimum age of earliest alveolar emergence varies quite a bit by sex and individual, with some people showing early signs in their mid-teens and others not until the late teens or early 20s. The takeaway: there is no single moment when wisdom teeth are "supposed" to come in. If yours are moving in your 20s, you're not late. You're normal.
What changes as you move deeper into your 20s is the available jaw space. By your mid-20s, your jaw is fully developed, which means a wisdom tooth that hasn't made it through yet is working against a fixed amount of room. That's when impaction becomes more likely, not because the tooth stopped growing, but because the space ran out.
If you're curious about what happens past your 20s, eruption can occasionally continue into the 30s and beyond, though it becomes less common. That means you may still be able to grow wisdom teeth at 30, especially if you were only noticing movement later than average eruption can occasionally continue into the 30s and beyond. The biology behind late eruption is worth understanding on its own terms.
What "growing in" actually looks like: full eruption vs. partial eruption vs. impaction
When most people say a wisdom tooth is "coming in," they picture something visibly breaking through the gum. That does happen, but it's only one version of the story. Clinically, there are a few distinct scenarios playing out in your 20s.
Full eruption

This is the best-case outcome. The tooth pushes all the way through the gum, aligns reasonably well, has enough space to function, and can be cleaned with a toothbrush. When this happens, the tooth often doesn't need to come out. The AAOMS is clear on this: if a wisdom tooth is fully erupted, painless, cavity-free, and surrounded by healthy gum tissue, extraction isn't automatically necessary.
Partial eruption
This is far more common and more problematic. The tooth breaks partway through the gum but doesn't fully emerge. A flap of gum tissue, called a gingival operculum or pericoronal flap, ends up draped over part of the tooth. That flap is nearly impossible to clean properly, which makes it a trap for food, bacteria, and inflammation. This is the setup for pericoronitis, one of the most common complications in young adults with wisdom teeth.
Impaction
An impacted wisdom tooth is one that can't break completely through the gum, usually because there isn't enough space. The tooth may be angled sideways (pressing into the adjacent second molar), tilted forward or backward, or stuck beneath the gum entirely. Impacted teeth can cause significant symptoms even when you can't see anything unusual in the mirror. In fact, some of the worst impaction symptoms come from teeth that are completely invisible to the naked eye.
Common symptoms and red flags in adults
The symptoms of an erupting or impacted wisdom tooth in your 20s range from mild annoyance to genuine medical urgency. Here's how to read what you're feeling.
Typical symptoms of eruption
- Dull pressure or aching at the very back of the jaw, sometimes radiating toward the ear
- Swollen or tender gum tissue behind the last visible molar
- Mild difficulty opening your mouth all the way
- Sensitivity when biting down in the back of the mouth
- A small visible bump or white point of tooth trying to poke through
- Feeling like your teeth are slightly more crowded than before
Red flags that need prompt attention
These symptoms suggest you've moved beyond normal eruption discomfort and into pericoronitis (infection of the gum tissue around a partially erupted tooth) or something more serious. The Cleveland Clinic advises scheduling a dentist appointment right away if you notice any of these:
- Throbbing pain that isn't improving or is getting worse
- Visible pus or a bad taste coming from the back of your mouth
- Noticeable swelling in your cheek, jaw, or face
- Fever
- Difficulty opening your mouth (trismus/lockjaw)
- Bad breath that doesn't respond to brushing
- Swollen lymph nodes under the jaw or in the neck
Go to an emergency room or urgent care rather than waiting for a routine dental appointment if you develop difficulty swallowing, a change in your voice, significant facial asymmetry, or any sign of breathing difficulty. These can signal a spreading deep-space infection, which is a genuine medical emergency. StatPearls identifies these as red-flag features of odontogenic infections that require urgent evaluation. Don't wait those out.
How dentists confirm what's happening: the exam and X-ray process

You can't properly assess a wisdom tooth situation just by looking in a mirror. Dentists piece together the picture using two main tools: a clinical exam and radiographic imaging.
The clinical exam
Your dentist will visually inspect the back of your mouth and probe the gum tissue around the area where the wisdom tooth is (or should be). They're looking for swelling, the presence of a pericoronal flap, signs of infection like pus or redness, and any effects on neighboring teeth. This gives them the functional picture, but it doesn't tell them where the tooth actually is, how it's angled, or whether it has any chance of erupting fully.
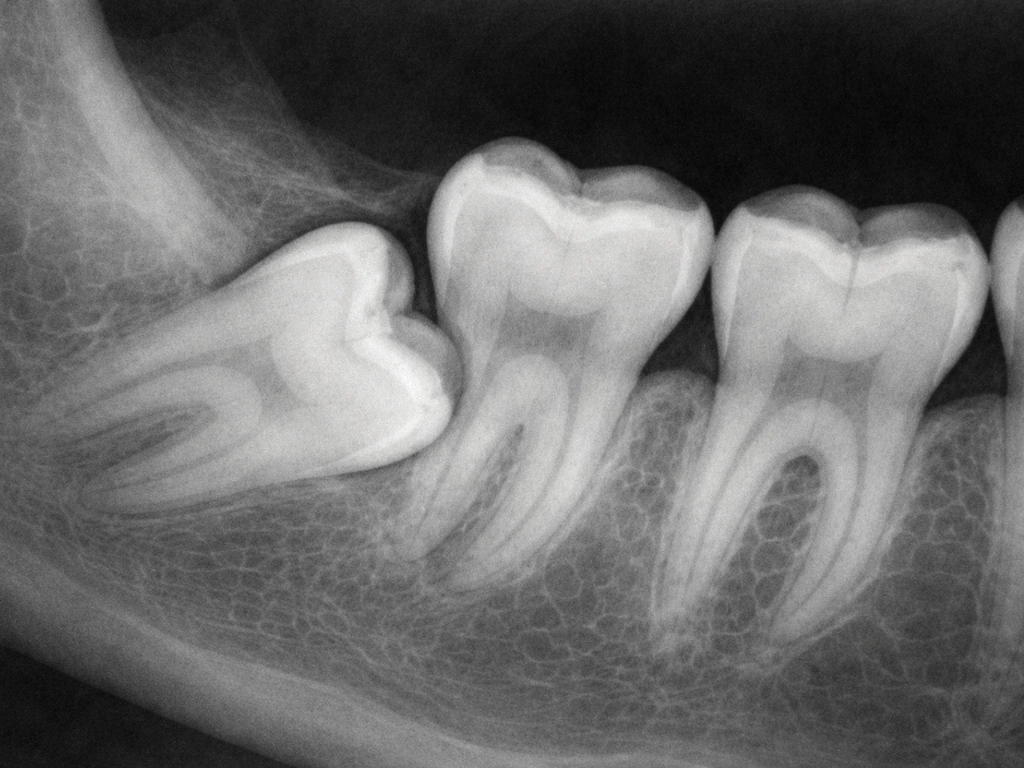
Panoramic X-rays (OPG)
A panoramic radiograph, sometimes called an OPG, is the standard first-line imaging tool for wisdom teeth. It produces a single image of your entire mouth, including all four wisdom teeth, both jaws, the roots, and the surrounding bone. It shows the tooth's exact position, the angle it's traveling, how close it is to the inferior alveolar nerve, and whether it has enough space to erupt.
The AAOMS includes impacted teeth explicitly on the list of clinical situations where radiographic imaging is indicated. For impacted third molars, AAOMS provides clinical guidance on management, including how to think about extraction versus monitoring and what imaging and approach considerations apply AAOMS clinical guidance on management of impacted third molars.
Most dentists will order one of these before making any management decision.
CBCT (cone beam CT) when needed
A cone beam CT scan produces a 3D image of the area, which is more detailed than a panoramic X-ray. It's not the default tool for every wisdom tooth case, but it becomes relevant when a 2D image shows the tooth is very close to the inferior alveolar nerve, or when the surgeon needs precise spatial information to plan a complex extraction. Updated ADA imaging guidance confirms that panoramic X-rays should be the initial assessment tool, with CBCT reserved for cases where there's a specific clinical need. The higher radiation dose of CBCT means it's used selectively, not routinely.
What to expect if wisdom teeth erupt in your 20s
There are really three paths the situation can take, and knowing which one you're on changes everything about how you manage it.
| Scenario | What it means | Likely outcome |
|---|---|---|
| Full, clean eruption | Tooth comes through completely, has adequate space, healthy gum tissue | Monitor and maintain; extraction often not needed |
| Partial eruption with pericoronal flap | Tooth partly visible, gum flap covering part of it, hard to clean | Recurring inflammation or pericoronitis; likely extraction eventually |
| True impaction (not erupting) | Tooth is stuck beneath the gum or bone, angulated, no path to emerge | Extraction usually indicated, especially if causing symptoms or damaging adjacent tooth |
The Mayo Clinic notes that when an impacted wisdom tooth pushes against the second molar, it can damage that neighboring tooth and increase infection risk in the area. This is a real consequence that many people don't consider until a dentist flags it on an X-ray. A tooth you can't see or feel can still be silently causing harm.
Research tracking asymptomatic impacted wisdom teeth over time has shown that somewhere between 30% and 60% of patients with initially symptom-free impacted teeth will develop problems over time. That's a wide range, and it reflects genuine clinical uncertainty, which is exactly why ongoing monitoring matters even when you feel fine.
Treatment and management options: from home care to extraction
Management isn't one-size-fits-all. What's right for you depends on whether the tooth is fully erupted, partially erupted, or impacted, and whether you're dealing with active symptoms, infection, or just monitoring.
Watchful waiting and monitoring
If your wisdom tooth is erupting without causing problems, and X-rays suggest it has a reasonable path to full emergence, a dentist may recommend monitoring it over time rather than rushing to extract. This is a legitimate option, but it comes with a responsibility: you need to actually go back for those follow-up appointments. An impacted tooth that looks fine at 22 may look very different at 26.
Home care and hygiene
If a wisdom tooth is partially erupted and not causing active infection, good oral hygiene is critical. Gently brush the area with a soft-bristled brush. Rinsing with warm salt water can reduce inflammation and keep the area clean. Chlorhexidine mouthrinse has evidence behind it for reducing complications in the context of wisdom tooth issues. Your dentist may recommend it specifically for managing mild pericoronal inflammation.
Pain relief
Over-the-counter pain relievers are the appropriate first line for managing eruption discomfort. The ADA recommends acetaminophen or ibuprofen for dental pain rather than jumping to antibiotics. Antibiotics are not a substitute for dental treatment, and they're not appropriate for every wisdom tooth situation. The ADA's antibiotic stewardship guidance is very clear on this: overuse of antibiotics does real harm, and most routine dental pain situations don't meet the criteria for antibiotic prescribing.
Treatment for pericoronitis
If you've developed pericoronitis, treatment typically involves professional cleaning of the area under the gum flap to remove trapped debris and bacteria. In some cases, a dentist may prescribe antibiotics if the infection has spread beyond the local tissue, though this is situation-dependent. For recurring pericoronitis, two surgical options exist: operculectomy (removing the gum flap itself) or extraction of the wisdom tooth. The Cleveland Clinic notes that monitoring is sufficient for some patients, while others need surgery to address the underlying anatomy.
Wisdom tooth extraction
Extraction becomes the recommended option when: the tooth is impacted with no path to erupt, there's damage or risk to the adjacent second molar, pericoronitis keeps coming back, the tooth has developed decay that can't be treated, or there's significant periodontal disease around the area. Cochrane evidence shows that antibiotics given around the time of extraction can reduce post-surgical infectious complications, though their use is still context-dependent and not automatic. Your oral surgeon will discuss what's appropriate based on your specific situation.
Myths about tooth regrowth and what's actually happening here
Here's something worth clearing up, because this site gets a lot of questions about it: wisdom teeth erupting in your 20s are not your body regrowing a tooth. They're not replacement teeth, and they're not a second chance for teeth you've lost elsewhere. They're your third set of molars, which were always there, just buried in your jaw, developing on a slow schedule that ends in your late teens or 20s.
Human adults get one set of permanent teeth. Once a permanent tooth is lost, your body has no biological mechanism to replace it. There are no stem-cell tooth fairy stories coming true yet in clinical dentistry, at least not as of today. Wisdom teeth are the last of your permanent teeth to erupt, but they are part of that original set. Their late arrival can feel surprising, especially if you assumed your teeth were "done" growing by your late teens, but they don't represent regeneration of anything.
Similarly, gum tissue that recedes doesn't grow back on its own, enamel that wears down doesn't regenerate, and a root that resorbs doesn't rebuild itself. The human dental system is genuinely limited in what it can repair. Wisdom tooth eruption is one of the very few instances where something new appears in your mouth as an adult, and even that process is just the completion of development that started in childhood, not actual regrowth.
So if you've been Googling whether your wisdom tooth coming in means your body can regenerate teeth, the answer is no. The two things aren't connected. What you're experiencing is normal developmental biology, not regeneration.
What to do right now: your next steps
If you're in your 20s and noticing back-of-mouth pressure, soreness, or swelling, here's the practical path forward.
- Book a dental appointment if you haven't had a recent exam and X-rays. Don't wait for the pain to get worse before making the call.
- Ask your dentist specifically for a panoramic X-ray if wisdom teeth haven't been evaluated recently. This is the standard first-line imaging for this situation.
- Manage mild discomfort at home with ibuprofen or acetaminophen, warm salt water rinses, and gentle brushing of the area.
- Do not self-diagnose with antibiotics or assume antibiotics from a previous prescription will solve the problem. They won't address the underlying anatomy.
- Go to urgent care or an emergency room without waiting if you develop fever, facial swelling, difficulty opening your mouth, or any trouble swallowing or breathing.
- Ask your dentist these questions at the appointment: Is the tooth erupting, partially erupted, or impacted? Is there enough space for it to come in fully? Is it affecting the second molar? What are my options: monitoring, cleaning, or extraction? What are the risks of waiting?
The good news about dealing with wisdom teeth in your 20s is that you're at the right age to address them proactively. Bone density and healing capacity are on your side. If extraction is needed, recovery is generally faster and more predictable in your 20s than in your 30s or 40s. If you're wondering can wisdom teeth grow in your 40s, remember that recovery and eruption patterns are usually less predictable than what you see in your 20s.
If you're in your 20s and curious about later eruption, note that the eruption window can still extend beyond 25 in some cases, so answers like can wisdom teeth grow after 25 are worth reviewing can wisdom teeth grow in your 40s. Getting a clear picture now, with a proper exam and X-rays, puts you in control of whatever comes next.
FAQ
If my wisdom tooth is starting to hurt, how fast do I need to see a dentist?
In most cases, the safest next move is to book a dental visit promptly, not to self-treat for weeks. If pain is mild, you can manage it briefly with ibuprofen or acetaminophen, warm salt-water rinses, and careful brushing around the back area, then get evaluated within days.
Can I tell whether my wisdom tooth is impacted just by looking in the mirror?
A mirror check can miss the most important situations, especially fully covered or sideways impacted teeth. Ask for imaging (usually a panoramic X-ray first) if you have persistent back-of-mouth pressure, recurring bad taste, or swelling even when you cannot clearly see a tooth coming through.
Why do my wisdom-tooth symptoms keep coming back even though they seem to calm down?
Yes. If the gum flap is covering part of a partially erupted tooth, food can pack under it and keep triggering inflammation, even if there is no obvious swelling on the outside. Look for recurring symptoms like intermittent soreness, bleeding when brushing that area, or periodic foul taste as a sign you need targeted treatment.
Is it okay to use a water flosser or hard rinsing to clean around a partially erupted wisdom tooth?
When the tooth is difficult to clean under a pericoronal flap, water-pick use can sometimes worsen irritation if you blast directly at the gum line. If you use one at all, keep pressure low, aim gently away from the flap, and rely primarily on a soft brush plus dentist-guided rinses.
Do I always need antibiotics for wisdom-tooth pain or pericoronitis?
Red, swollen gums around a partially erupted tooth can be managed locally at first, but antibiotics are not automatically needed. Antibiotics are generally reserved for cases with clear spread beyond the local gum tissue or systemic signs, so don’t request them without an exam.
If I’m told to monitor it, what are the risks of waiting?
Try not to delay because of fear of extraction. In your 20s, extraction is often more predictable, and earlier management can prevent damage to the adjacent second molar or repeated infections. If your dentist recommends monitoring, schedule follow-ups, since tooth position and gum health can change over months.
What symptoms mean this could be an emergency, not just normal eruption discomfort?
Emergency signs include difficulty swallowing, voice changes, facial swelling with asymmetry, fever, or any breathing trouble. These can indicate a spreading deep-space infection, where urgent in-person care is needed rather than waiting for a routine appointment.
If my wisdom tooth erupts normally and doesn’t hurt, does that mean I can ignore it?
If a wisdom tooth is fully erupted, painless, not decayed, and surrounded by healthy gum tissue, it may be monitored rather than extracted. The key distinction is that “no pain” alone is not enough, the gum health and tooth status on imaging matter.
What are examples of wisdom-tooth problems that don’t show obvious changes in my mouth?
Sometimes a wisdom tooth can cause problems even when it looks normal. Common examples are occasional gum flap inflammation, trapping of food under partially covered tissue, or pressure against the second molar that doesn’t cause dramatic symptoms until later. Imaging helps catch these patterns early.
What can I do at home between dentist visits if I’m getting pericoronitis?
If you have swelling, bad taste, or recurring inflammation, improve cleaning in the back area with gentle brushing and prescribed mouthrinse, and rinse with warm salt water. If your dentist recommends operculectomy or extraction for recurring pericoronitis, consider addressing the source because home care alone often can’t eliminate the trapped area.
How can I be sure the pain is from the wisdom tooth and not another tooth or gum problem?
It is possible for symptoms to be caused by something else, like a cavity on the second molar, gum disease, or an unrelated infection. If the pain is localized to the back but imaging shows no active wisdom-tooth issue, ask your dentist what tooth and gum area is actually responsible.
What questions should I ask at my appointment to understand my imaging results and options?
Make sure your dentist explains the plan for imaging and follow-up. Ask whether you need only a panoramic X-ray or whether a 3D scan is justified due to proximity to the nerve or complex positioning, and confirm when you should return if you choose monitoring.
Next Articles

Can Wisdom Teeth Grow in Your 30s? Symptoms, Timing, Options
Can wisdom teeth erupt in your 30s? Learn symptoms, timing, how dentists confirm, and when extraction is needed.

Do Milk Teeth Grow Back? Timelines, What to Do, Red Flags
Learn if milk teeth regrow, typical timelines for permanent teeth, what to do after loss or injury, and red flags.

Can Milk Teeth Grow Twice? Replacement vs True Regrowth
Can milk teeth grow twice? Learn why baby teeth usually only get replaced, not regrown, and what to do if one falls out