When people say an "ovarian cyst grows teeth," they're almost always talking about a mature cystic teratoma, also called a dermoid cyst. This is a benign germ-cell tumor that can contain hair, skin, fat, bone, and yes, sometimes tooth-like structures. It is not a regular ovarian cyst that spontaneously sprouted a molar. It's a specific type of growth built from cells that retain the ability to differentiate into almost any tissue in the body, including the materials that make up teeth. Understanding the difference between that biological quirk and the idea that "human teeth can grow back" is exactly what this article is here to sort out.
Why Do Ovarian Cysts Grow Teeth? What Really Happens

Marcus Holloway
4 May 2026

The "ovarian cyst grows teeth" myth vs. what's actually happening
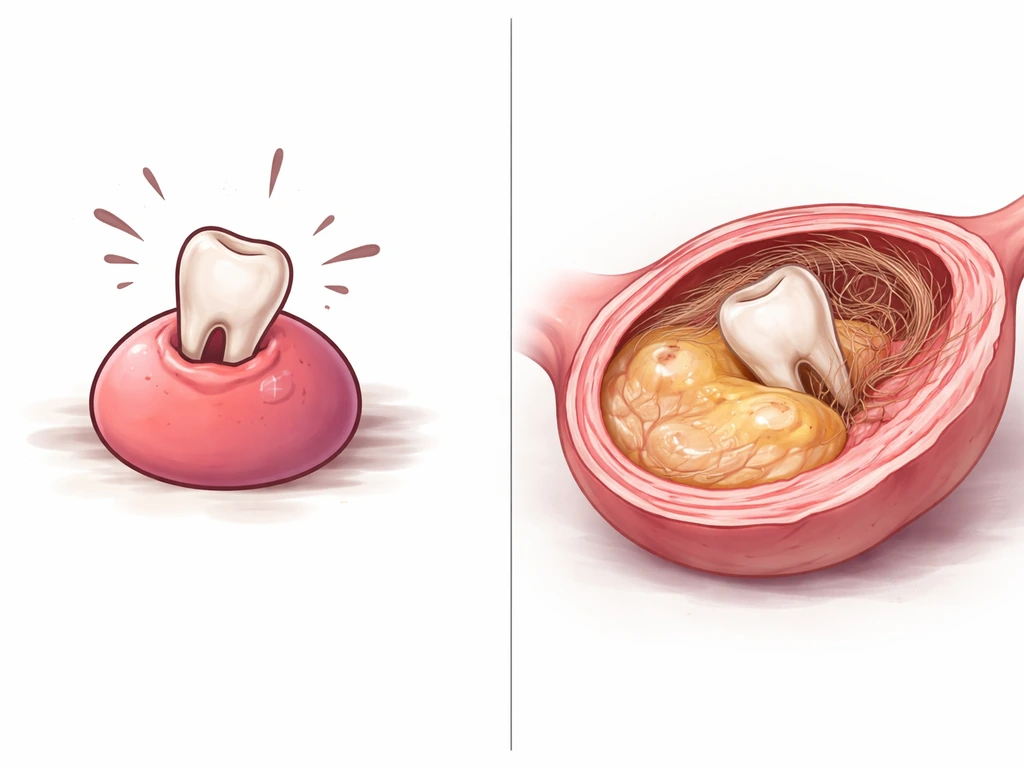
The phrase gets thrown around in a way that makes it sound like a normal ovarian cyst somehow decided to manufacture a tooth. That's not what's going on. Ordinary functional ovarian cysts, like follicular cysts or corpus luteum cysts, are fluid-filled sacs related to the normal ovulation cycle. Cleveland Clinic explains that ovarian dermoid cysts are fluid-filled sacs containing tissue such as hair, skin, teeth, and other body parts, and that cysts may be removed if there is concern about rupture, torsion, or cancer risk. They do not contain teeth, hair, or bone. When you see teeth mentioned alongside an ovarian finding, clinicians are almost certainly looking at a mature cystic teratoma, which is an entirely different category of growth.
The confusion is understandable because the word "cyst" gets used loosely. Dermoid cysts and teratomas are technically tumors, though the word "tumor" alone sounds scarier than the situation usually warrants. The vast majority of mature cystic teratomas are benign. The American College of Obstetricians and Gynecologists (ACOG) classifies them this way, and the clinical evidence strongly supports it. The headline-grabbing detail, the teeth, is a real pathological finding, just not evidence of anything regenerative or supernatural.
What teratomas actually are and why teeth can form inside them
A mature cystic teratoma forms from a type of cell called a germ cell. Germ cells are essentially the body's most pluripotent cells: they carry the genetic instructions to build an entire organism. Under normal circumstances, they develop into eggs or sperm. But occasionally, one of these cells begins differentiating on its own without fertilization. Because it has instructions for building all types of tissue, it can produce structures from any of the three embryonic germ layers: ectoderm, mesoderm, and endoderm. Teeth are ectodermal and mesodermal in origin, which is exactly why dental tissue can appear inside these tumors.
StatPearls (NIH/NCBI) describes mature cystic teratomas as containing well-differentiated tissues derived from all three germ cell layers, which can include skin, hair follicles, sebaceous glands, fat, cartilage, bone, thyroid tissue, and tooth-like structures. The "tooth" found in a teratoma is not an isolated anomaly. It is the predictable output of a cell that was programmed to potentially build an entire body deciding to do just that in a very localized, disorganized way.
On imaging, clinicians often look for what's called the Rokitansky nodule, sometimes called the dermoid plug. This is a dense mural nodule within the cyst wall, and it is where tooth-like calcifications and ossification tend to cluster. Radiology references specifically describe this region as the most characteristic location for dental or calcific components, and it is highly recognizable on both ultrasound and CT.
These are not "real teeth" in any regenerative sense

This is where the site's core question intersects directly with ovarian teratomas. People sometimes hear "teeth in an ovarian cyst" and wonder: does this mean the human body can grow new teeth after all? This is why the rumor behind can worms grow in your teeth is so misleading, since teeth do not come from random tissue growth in the mouth human body can grow new teeth. The answer is no, and here's why that matters.
Functional tooth formation in the mouth requires a coordinated developmental sequence: dental epithelium and mesenchyme must interact in a specific spatiotemporal pattern to build enamel, dentin, pulp, cementum, and the periodontal ligament. The tooth structures inside a teratoma go through a version of this process, but in a completely disorganized environment, without proper orientation, without functional occlusion, and often with structural defects. In other words, these cysts grow teeth because germ cells can differentiate into tooth-forming tissues during tumor development dermoid cysts grow teeth. Histological studies have found that teratoma-derived teeth frequently show enamel hypoplasia, fluorosis-like changes, and caries-like lesions. They are developmental artifacts, not functional dental organs.
More importantly, enamel, the outermost layer of a real tooth, is acellular after it forms. That means once enamel is made, the cells that produced it (ameloblasts) are gone. There is no repair mechanism, and current research confirms that functional enamel regeneration has not been demonstrated in humans in any clinical trial. Teratoma teeth do not change that reality.
They are not evidence that your mouth could grow a third set of molars. They are products of embryonic programming running in the wrong location, without the structural context that makes a tooth useful. The biology that makes dermoid cysts grow teeth is related to, but completely distinct from, any discussion of normal dental regeneration.
If you are trying to understand how tonsil stones grow, it helps to know that plaque, trapped debris, and bacteria can build up in the tonsil crypts over time The biology that makes dermoid cysts grow teeth.
If you're interested in how similar developmental biology plays out in other cyst-type structures, the same principle applies to dermoid cysts found in other parts of the body. The phenomenon of germ-cell-derived tissue appearing in unexpected anatomical locations is a broader concept that spans multiple tissue types.
Symptoms, diagnosis, and when to get evaluated urgently
Many mature cystic teratomas cause no symptoms at all and are found incidentally during a pelvic ultrasound done for another reason. When symptoms do appear, they tend to be vague: a dull ache or pressure in the lower abdomen, a sense of pelvic heaviness, or occasional bloating. Because these growths can displace the ovary and are often larger than typical functional cysts, they sometimes cause a dragging sensation on one side.
The two complications you really want to avoid are torsion and rupture. Torsion is when the ovary, weighed down or shifted by the cyst, twists on its own blood supply. Research on mature cystic teratoma surgical management indicates that torsion risk is highest for cysts above 5 to 6 cm, largely because these larger cysts create a longer pedicle that makes twisting more likely. Rupture carries a different risk: spilling the contents of a teratoma into the peritoneal cavity can cause a severe chemical peritonitis. Both scenarios are emergencies.
Symptoms that mean you need emergency care today
- Sudden, severe one-sided pelvic or lower abdominal pain that doesn't improve within minutes
- Pain accompanied by nausea and vomiting, particularly if it comes on abruptly
- Fever combined with pelvic pain
- Feeling faint, dizzy, or lightheaded alongside pelvic pain
- Rapid worsening of pain over a short period
The Cleveland Clinic advises seeking emergency care immediately for sudden severe symptoms like these. If you're managing a known dermoid cyst and this type of pain hits, do not wait to call your OB. Go to the emergency room.
How doctors diagnose a dermoid cyst or teratoma

Pelvic ultrasound is usually the first and most practical tool. The classic ultrasound features of a mature teratoma are fairly distinctive: a densely echogenic Rokitansky nodule with posterior acoustic shadowing, echogenic lines and dots (sometimes called dermoid mesh, caused by hair within the cyst), and a "tip of the iceberg" appearance where the front wall is visible but the back is obscured by shadowing. If the ultrasound is inconclusive, a CT scan can confirm the diagnosis by clearly showing fat density and calcification, sometimes with a dentiform shape that looks unmistakably like a tooth. MRI is used when further soft-tissue detail is needed. Final confirmation is histological, meaning the pathologist examines the tissue after removal and identifies the component layers.
Treatment options: surgery, surveillance, and how size changes the math
Not every dermoid cyst needs immediate surgery. ACOG's framework for ovarian cyst management considers size, symptoms, the patient's age, and fertility goals before recommending a course of action. For small, asymptomatic teratomas, a watchful waiting approach with periodic ultrasound surveillance is reasonable. Prospective data from one study estimated the growth rate of mature cystic teratomas at approximately 1.5 to 1.7 mm per year, which means a 3 cm cyst in a young asymptomatic woman is not necessarily racing toward a crisis.
Surgery becomes strongly recommended when the cyst is large (generally above 5 to 6 cm given the torsion data), symptomatic, growing noticeably on serial imaging, or when the diagnosis is uncertain. The preferred surgical approach for a benign teratoma is laparoscopic cystectomy, where the cyst is removed while the ovary is preserved. This is especially important for younger women and those who want to preserve fertility. Oophorectomy (removing the whole ovary) is sometimes necessary when the ovary is too damaged to salvage, particularly in torsion cases where the blood supply has been cut off for too long.
| Factor | Watchful Waiting | Surgery |
|---|---|---|
| Cyst size | Under 5 cm, not growing | 5 cm or larger, or rapidly growing |
| Symptoms | None or very mild | Persistent pain, pressure, acute symptoms |
| Torsion or rupture risk | Low (small, stable) | Elevated (large, displaced ovary) |
| Imaging certainty | Classic benign features confirmed | Atypical features, uncertainty about malignancy |
| Fertility considerations | Preserve ovarian tissue with surveillance | Cystectomy preferred over oophorectomy when possible |
| Patient preference | Comfortable with monitoring | Prefers definitive removal |
For the rare cases where a teratoma shows immature (fetal-type) tissue rather than adult-type tissue, or if there is any concern for malignant transformation, the NCI's treatment guidelines describe surgery as the standard first step, often followed by staging and potentially chemotherapy. But this applies to immature teratomas and malignant germ-cell tumors, not to the typical mature cystic teratoma that most people are dealing with when they hear the phrase "ovarian cyst with teeth."
Prognosis, recurrence, and long-term follow-up
The good news is that mature cystic teratomas are overwhelmingly benign and surgical outcomes are excellent, especially when the ovary can be preserved. The less-great news is that recurrence is a real possibility, particularly for younger women.
A five-year recurrence study in young women found that among 372 patients who had cystectomy, recurrence rates were meaningfully tracked over time. A separate 10-year cumulative recurrence analysis reported rates around 38% in young women with mature cystic teratoma after surgery. Predictive factors for recurrence include younger age (under 30), a larger initial cyst size (8 cm or more), and bilateral cysts at the time of surgery. This doesn't mean recurrence is inevitable, but it does mean that follow-up ultrasounds are not optional.
Fertility preservation is a central goal in surgical planning for reproductive-age patients. Laparoscopic cystectomy has a strong track record for preserving ovarian function. The concern is damage to healthy ovarian tissue, particularly primordial follicles, during the dissection. A careful, experienced surgeon and a well-timed intervention (before the cyst enlarges to the point of extensive ovarian damage) are both important factors.
Practical questions to bring to your clinician
- What is the current size of the cyst, and how does that affect the torsion or rupture risk for me specifically?
- How often should I get follow-up ultrasounds if we're taking a watchful waiting approach?
- Is the imaging appearance classic for a mature teratoma, or are there any atypical features that need further workup?
- If I need surgery, what is the plan for preserving my ovarian tissue and fertility?
- What are the signs that I should go to the emergency room before my next scheduled appointment?
- Given my age and cyst characteristics, what is my estimated recurrence risk, and what is the follow-up plan after surgery?
One more thing worth saying plainly: if you came to this article because you saw "ovarian cyst with teeth" somewhere and it alarmed you, that reaction makes sense. It is a genuinely striking finding. But it is not evidence that something profoundly wrong is happening, and it is absolutely not evidence that the human body can regenerate teeth normally. People often wonder whether can tonsil stones grow overnight, but they usually build up gradually from trapped debris and bacteria.
Teratomas form because of a very specific quirk of germ-cell biology. Your dentist is not going to find a surprise molar growing in because your body "learned" something from your ovarian cyst. The two things are biologically unrelated. What you need is a good pelvic ultrasound, a conversation with your OB or gynecologist about size and symptoms, and a follow-up plan.
That's the practical path forward.
FAQ
If a doctor says “dermoid cyst” or “mature cystic teratoma,” does that automatically mean it contains teeth?
Not always. Many mature teratomas have calcifications or fat, but the “tooth” description depends on what the imaging or pathology actually shows. A report may say hair, fat, or a calcified focus without explicitly calling out teeth.
Can an “ovarian cyst with teeth” be cancer?
Most mature cystic teratomas are benign. Cancer concern usually relates to unusual imaging features or pathology results, such as immature tissue or other high-risk histology. If the report raises those flags, treatment planning typically changes and surgery is handled as the first step.
Why do some reports mention a “Rokitansky nodule” or “dermoid plug,” and does that affect treatment?
That nodule is where the dense components, often including calcifications, tend to cluster. While it helps confirm the diagnosis on ultrasound or CT, the decision to operate is usually driven by size, symptoms, growth over time, and torsion risk, not just the nodule itself.
How do I know whether my cyst is a functional cyst versus a dermoid/teratoma?
Functional cysts follow ovulation patterns and are usually fluid-dominant and temporary. Dermoid/teratomas tend to contain fat, calcifications, and characteristic echogenic patterns on ultrasound. The imaging wording and follow-up interval matter, so ask what features made the clinician categorize it as dermoid.
If I have no symptoms, should I still remove a mature teratoma?
Often you can consider surveillance, especially when the cyst is small and imaging is clearly consistent with a mature teratoma. The key decision points are cyst size (torsion risk increases as size rises), any growth on serial scans, and your age and fertility plans.
What symptoms mean I should treat this as an emergency rather than “wait and see”?
Sudden, severe one-sided pelvic pain (torsion) or sudden worsening pain with systemic symptoms (possible rupture) warrants emergency evaluation. Mild, vague pressure that slowly increases may be less urgent, but any abrupt escalation should be checked immediately.
Does “watchful waiting” mean ultrasounds are optional?
No. Even though mature teratomas often grow slowly, follow-up imaging is how clinicians monitor for enlargement and changing risk. Skipping surveillance reduces your ability to catch growth patterns or new concerning features early.
If I’m trying to preserve fertility, is laparoscopic cystectomy always the best choice?
It is commonly preferred for benign mature teratomas because it aims to remove the cyst while preserving ovarian tissue. However, the best approach depends on how much the cyst has damaged the ovary, the surgical findings, and whether torsion has already compromised blood supply.
What increases the chance of recurrence after cyst removal?
Recurrence risk is higher in younger patients, with larger cysts at the time of surgery, and with bilateral disease. Your surgeon will usually tailor the follow-up schedule based on these factors.
If teeth are found in the cyst, will that change my dental care or require special treatment?
No. Dental tissue inside a teratoma does not translate to any regenerative capability in the mouth. Your ongoing dental needs are handled as usual, based on oral hygiene and standard preventive or restorative care.
What should I ask my OB or gynecologist at my next visit?
Ask for the exact diagnosis term from the imaging report (for example, mature cystic teratoma), the cyst size in centimeters, whether there are fat or calcification findings, whether there is any concern for immature tissue, and the planned follow-up interval. Also ask what symptoms would trigger urgent care in your specific case.
Next Articles

How Do Dermoid Cysts Grow Teeth? Causes, Symptoms, Treatment
Learn how dermoid cysts can form tooth-like material, what symptoms appear, and how doctors diagnose and treat them.

How Do Tonsil Stones Grow? Timeline and Recurrence Explained
Explains how tonsil stones form in crypts, how long growth takes, why they recur, and what to do for faster relief.

Do Milk Teeth Grow Back? Timelines, What to Do, Red Flags
Learn if milk teeth regrow, typical timelines for permanent teeth, what to do after loss or injury, and red flags.