Yes, wisdom teeth do grow in spurts. You might feel nothing for months, then wake up one week with a sore jaw, pressure at the back of your mouth, and swollen gum tissue, only for it to calm down again a few weeks later. That stop-start pattern is completely normal during eruption. What matters is knowing when the pain is just a tooth moving through gum tissue versus when it is a sign of impaction or infection that actually needs a dentist.
Do Wisdom Teeth Grow in Spurts? Eruption Timeline and What to Do

Marcus Holloway
13 May 2026

What 'spurts' actually look like with wisdom tooth eruption

When people say a wisdom tooth is growing in spurts, they are describing something real: the tooth moves in phases rather than in one smooth, continuous push. During an active phase, the crown edges its way through the jawbone and then through the overlying gum tissue. Pressure builds, the gum gets irritated or slightly torn, and you feel it as soreness, throbbing, or a sense of fullness at the back of your mouth. Then the tooth pauses. The gum heals around wherever the tooth stopped, the inflammation settles, and things feel fine again, sometimes for weeks or months.
These pauses are not the tooth resting in some planned biological sense. They reflect the balance between the forces pushing the tooth upward and the resistance from surrounding bone, gum tissue, and neighboring teeth. When conditions favor movement again, eruption resumes and symptoms return. This is why so many people describe wisdom teeth as 'coming and going' for a year or more before the tooth is fully through, partially through, or definitively stuck.
One thing worth clearing up right away: eruption is not the same as regrowth. The tooth was always there, developing in the jaw since childhood. It is not generating new dental structure on demand. It is simply moving into position. Once it is in the mouth, enamel cannot replenish itself if it wears or chips, because the cells that built the enamel (ameloblasts) are gone by the time the tooth erupts. So 'growing in spurts' describes movement through tissue, not regeneration of tooth material.
Typical wisdom tooth timeline and why it varies so much
blank" rel="noopener noreferrer">Wisdom teeth, formally called third molars, are the last teeth to develop and erupt. Most people see them arrive somewhere between ages 17 and 25, though eruption can start earlier in some individuals and push into the late twenties or beyond in others. That timing is also one reason wisdom teeth can seem to “come and go” with symptoms for a while before they fully emerge why do wisdom teeth grow so late. The American Association of Oral and Maxillofacial Surgeons and the Merck Manual both use that 17 to 25 window as the standard reference range, but 'standard' covers a lot of variation.
Several factors explain why your timeline might look nothing like a friend's. Jaw size is a big one: if there is limited space behind the second molars, the wisdom tooth may only partially emerge before running out of room. The angle of the tooth in the bone matters too. A tooth that is tilting forward (mesioangular impaction) behaves very differently from one that is nearly vertical. Root development stage, the density of the overlying bone, and plain individual biology all play a role. Some people never develop wisdom teeth at all, which is covered elsewhere on this site. Others develop them but they stay completely buried, causing no symptoms whatsoever.
Why eruption can pause, restart, and suddenly hurt
The stop-start pattern has a few specific causes worth understanding, because they point toward very different outcomes.
Impaction and jaw space
When the jaw simply does not have enough room for the tooth to fully erupt, the tooth gets stuck, or impacted. It might poke partway through the gum and go no further. That partial eruption is where a lot of the trouble starts, because a partially erupted tooth creates a pocket between the tooth surface and the overlying gum flap (called an operculum) where bacteria collect and food debris accumulates. This sets the stage for infection.
Angulation
Dentists classify wisdom tooth angulation using systems like Winter's classification: vertical, horizontal, mesioangular (tilting toward the front of the mouth), distoangular (tilting toward the back), and others. A mesioangularly tilted tooth is essentially trying to push into the back of the second molar, which is why it so often gets stuck and causes pressure pain. The angulation also determines how complex any eventual removal would be.
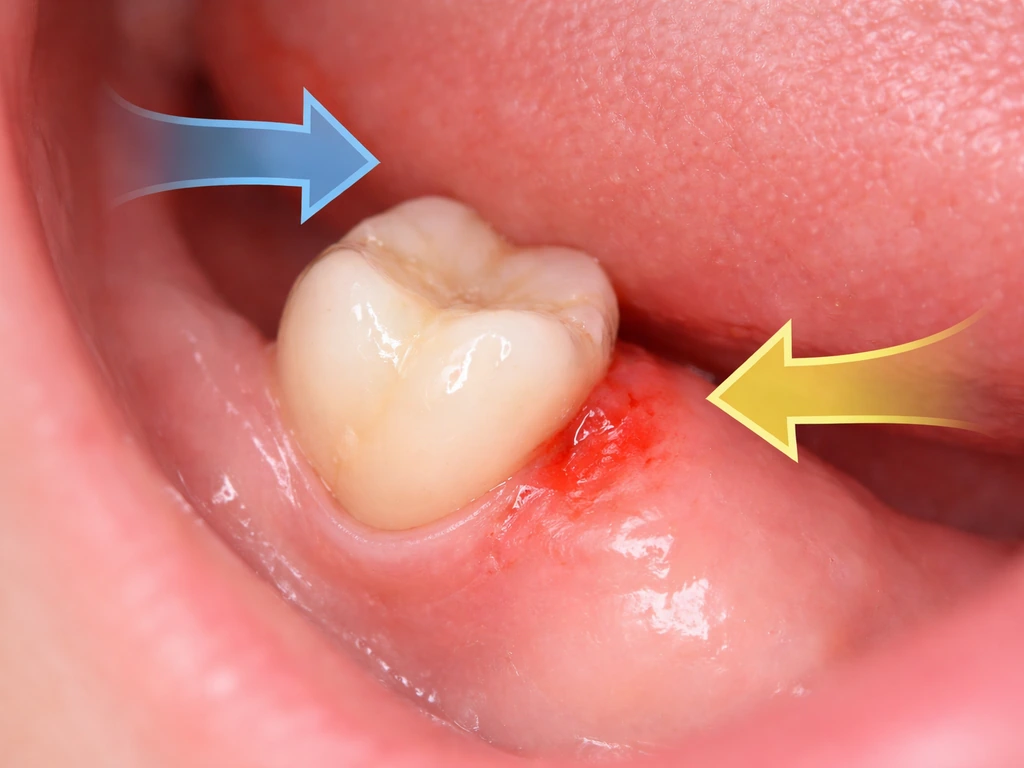
Pericoronitis: inflammation around the erupting tooth

Pericoronitis is the clinical name for infection and inflammation of the gum tissue surrounding a partially erupted tooth. It is extremely common with wisdom teeth and is one of the main reasons eruption feels like it comes in painful waves. Bacteria get under the gum flap, the tissue swells, it gets painful, sometimes it settles down on its own or with basic hygiene, and then it flares again. Mild pericoronitis typically causes localized pain and a swollen gum at the back of the mouth. More advanced cases bring in symptoms you should not ignore: fever, swelling of the face or jaw, difficulty opening your mouth fully (trismus), or difficulty swallowing.
Normal eruption symptoms vs. warning signs
Knowing what is expected versus what signals a problem makes a real difference in deciding whether to wait or book an appointment today.
| Likely normal eruption | See a dentist promptly |
|---|---|
| Mild soreness or pressure at the back of the mouth | Fever or chills alongside jaw pain |
| Gum tenderness that comes and goes over days or weeks | Difficulty opening your mouth more than a couple of fingers wide (trismus) |
| Slight swelling of the gum directly over the erupting tooth | Visible facial or jaw swelling that is spreading |
| Mild discomfort when biting down | Difficulty or pain when swallowing |
| A small amount of bleeding from the gum during eruption | Pus or persistent bad taste near the tooth |
| Pressure sensation radiating toward the ear or jaw | Pain that is severe, not improving, or waking you at night |
The warning signs in the right column can indicate that a pericoronitis infection is spreading beyond the local gum tissue into deeper spaces of the head and neck. StatPearls notes that symptoms like trismus, facial swelling, difficulty swallowing, voice changes, or breathing difficulty can mean infection has spread to adjacent spaces, which is a situation requiring urgent escalation, not home management.
How dentists figure out what is actually going on
A clinical exam can tell a lot. Your dentist will look at where the tooth sits, how much gum covers it, whether there is an active infection, and how easily your mouth opens. But the real picture comes from imaging. A panoramic X-ray (an OPG or orthopantomogram) is the standard first step for evaluating wisdom teeth. It shows the position of all four third molars, their angulation, the stage of root development, how much bone surrounds them, and whether there are any signs of pathology in the follicle around the tooth or bone loss near adjacent teeth.
Dentists use the panoramic image to assess several specific things: the depth of the tooth in alveolar bone, its inclination, the mesiodistal space available for eruption, marginal bone levels on the neighboring second molar, and any radiological signs of follicular pathology. This is exactly the kind of information that tells them whether a tooth has a realistic path to full eruption or whether it is stuck for good.
A cone beam CT (CBCT) scan gives a three-dimensional picture and is sometimes used when a panoramic X-ray suggests a high-risk situation, for example when a tooth appears very close to the inferior alveolar nerve. Current guidance is clear though: CBCT should only be used when the findings would genuinely change the risk assessment or treatment plan, not as a routine step for every third-molar evaluation.
What you can do right now: home care and pain management

If you are in the mild-to-moderate discomfort zone with no fever, no swelling beyond the gum, and no trouble opening your mouth, there are a few practical things you can do while you arrange a dental visit or wait out a minor flare.
- Rinse with warm saltwater several times a day, particularly after eating. This helps flush debris from the pocket around the tooth and reduces bacterial load.
- Chlorhexidine mouthwash (0.12% or 0.2% concentration depending on what is available) is recommended in clinical guidelines as part of first-line local management. Use it as directed, not as a long-term substitute for seeing a dentist.
- Take NSAIDs (such as ibuprofen) for pain, which is the primary recommended oral analgesic approach for pericoronitis-related discomfort. Follow standard dosing instructions and take with food.
- Keep the area as clean as possible. A soft-bristled toothbrush angled toward the gum line and gentle flossing (if accessible) helps prevent debris buildup under the gum flap.
- Avoid poking or pressing on the swollen gum. It will not help the tooth erupt faster and can introduce more bacteria.
- Book a dental appointment even if symptoms settle. A flare that resolves does not mean the underlying situation has changed.
If you have fever, spreading swelling, or difficulty opening your mouth, do not manage this at home. Those are signs of escalating infection and you need same-day dental or medical attention.
Treatment options: monitor, manage, or remove
There is no single right answer for every wisdom tooth, and the decision depends on what the tooth is doing, what symptoms you are having, and what imaging shows. Here is how the main paths break down.
Watchful waiting
If a wisdom tooth is erupting on a clear vertical path with adequate space and only mild intermittent symptoms, monitoring is a reasonable approach. Your dentist may recommend periodic X-rays to track progress and flag any early problems before they develop.
Managing pericoronitis without extraction
For a first episode of pericoronitis, the standard approach is local management: debridement and irrigation of the pericoronal space to clear out bacteria and debris, sometimes combined with chlorhexidine or hydrogen peroxide rinses. If the gum flap (operculum) is the persistent problem and the tooth is erupting vertically with space available, a minor procedure called an operculectomy, removing that flap of tissue, can resolve recurring flare-ups without extracting the tooth.
Antibiotics are not first-line treatment for pericoronitis. Clinical guidelines from Royal College of Surgeons England, NHS Scotland, and the HSE are consistent on this: antibiotics are indicated only when there is fever, spreading infection, severe localized infection that is not responding to local measures, or trismus. When prescribed, a short course (around three days) of amoxicillin, with or without metronidazole, is a typical regimen alongside local treatment, not as a replacement for it.
Extraction
Extraction becomes the conversation when a tooth is clearly impacted with no realistic path to full eruption, when pericoronitis has occurred more than once (after the acute infection has settled), or when there are other complications like cyst formation, damage to the adjacent second molar, abscesses, or cellulitis. NICE's guidance lists specific pathological indications for removal: cellulitis, abscess, osteomyelitis, follicular cyst or tumor, and cases where the tooth would obstruct necessary surgery or reconstruction. NICE also acknowledges that how much weight to give pericoronitis recurrence when deciding on removal is genuinely uncertain, which is part of why clinical judgment and your specific imaging matter so much.
Managing the opposing tooth
In some situations, if an upper wisdom tooth is biting down on or traumatizing an inflamed lower gum flap and causing repeated irritation, the opposing upper tooth may be adjusted or removed. Upper wisdom teeth can also erupt in phases, but they are usually described based on their position in the jaw and how much gum covers them upper wisdom teeth erupt. This is a less common approach but it does feature in the guidelines as a possible local management option.
Wisdom teeth vs. dental regeneration: what can and cannot actually regrow
This is worth addressing directly because it comes up a lot. A wisdom tooth erupting in spurts is not regenerating. It is a tooth that was already fully formed in the jaw, now pushing its way through bone and gum tissue. The movement is real and the discomfort is real, but the tooth itself is not growing new structure.
Once a wisdom tooth (or any permanent tooth) has erupted, it cannot regenerate enamel that has been lost to wear, acid erosion, or decay. The ameloblasts that built the enamel during tooth development are no longer present once the tooth comes into the mouth. Enamel has no cellular machinery to remodel or deposit new mineral from within, which is why enamel loss in adults is permanent. This is a well-established biological limit, not a gap in dental technology.
Similarly, a wisdom tooth that has been extracted does not grow back. Adults have one set of permanent teeth and there is no third dentition waiting in reserve. If you are wondering whether it is biologically possible to simply not develop wisdom teeth at all, that is a genuinely common variation, and some people are born without them entirely.
What can happen, and what sometimes confuses people, is that a partially erupted or impacted tooth may not be obvious on a visual exam, so a tooth that 'suddenly appears' might feel like a new arrival when it has actually been sitting just below the gumline for years. That is still just eruption, not regeneration. The eruption-in-spurts pattern can make it feel dramatic and new, but biologically it is the same tooth that has been developing in your jaw since you were a child.
The bottom line: if your wisdom teeth are causing symptoms that come and go, that is normal eruption biology at work. Get a panoramic X-ray so you and your dentist can see exactly what is happening below the gumline, manage symptoms with saltwater rinses and NSAIDs in the meantime, and take seriously any symptoms like fever, jaw stiffness, or facial swelling. Those are the signs that home management is not enough and that the clock on getting professional care starts now.
FAQ
How long do wisdom teeth “spurts” usually last before the pain settles again?
A flare can calm down in days to a couple of weeks, but the overall stop-start pattern commonly continues for months. The exact length depends on whether the tooth has space to erupt and whether pericoronitis is repeatedly triggered by food and bacteria under the gum flap.
Is it normal for symptoms to disappear for months, and then come back?
Yes, intermittent symptoms can be normal during eruption because the tooth alternates between active movement and pauses while gum tissue heals. Symptoms that return more severely, last longer each time, or start spreading beyond the gumline are not the usual pattern and should be assessed.
Does a “spurting” wisdom tooth mean it is close to fully erupting?
Not necessarily. Sometimes the tooth makes progress and then gets stuck again due to limited space or angulation. Progress is hard to judge by pain alone, so imaging (usually a panoramic X-ray) is the reliable way to see where the crown and roots really are.
What are the signs my pain is pericoronitis rather than normal eruption pressure?
Pericoronitis often comes with gum flap swelling at the back of the mouth, bad taste or odor, pain that feels localized to the gum over the tooth, and episodes that flare after meals. Normal eruption pressure is more generalized and tends to improve without developing a repeatedly inflamed gum flap.
If I have mild symptoms, when should I stop waiting and call the dentist?
Call promptly if pain keeps recurring over multiple weeks, you are developing difficulty chewing, you notice pus or increasing swelling, or you cannot keep the area clean with normal brushing. Waiting is reasonable only when symptoms are mild, you have no fever, and the pattern is not worsening.
Can I use hydrogen peroxide or chlorhexidine rinses safely while I wait?
They can be helpful for short-term local control, but follow your dentist or package directions, avoid prolonged use without guidance, and stop if you get irritation or a worsening burning sensation. Overuse of strong antiseptics can irritate already inflamed tissue.
What pain medicines are typically safest for wisdom tooth discomfort?
NSAIDs like ibuprofen often work well for inflammation and pain, but avoid them if you have a medical reason you cannot take NSAIDs (such as certain stomach or kidney conditions). If you use acetaminophen, keep within label dosing limits and do not combine products that contain the same ingredient.
Should I try to push the gum flap or clean under it with a tool?
No. Prodding the operculum or digging under the gum flap can worsen inflammation and increase bleeding or infection risk. Safe options are gentle saltwater rinses and normal oral hygiene, and if irrigation or debridement is needed, it should be done by a dental professional.
Why do some wisdom teeth cause pain but others never bother me?
Symptoms depend on position, angulation, and space, plus whether food and bacteria get trapped under a partially erupted operculum. Teeth that erupt vertically with enough room may cause little or no pericoronitis, while tilted or partially covered teeth are more likely to trigger recurrent inflammation.
Will a panoramic X-ray be enough, or do I need a CBCT scan?
Often a panoramic X-ray is the first step because it shows tooth position, angulation, and relationship to adjacent teeth. CBCT is usually reserved for higher-risk situations where 3D detail would change the plan, such as when a tooth appears very close to a nerve, because it is not typically done for every case.
Could the pain be from something else like a cavity or gum infection?
Yes. A sore back tooth area can come from decay on the second molar, periodontal problems, or food impaction unrelated to the wisdom tooth. That is another reason to get assessed, especially if the pain is one-sided, persistent, or not clearly tied to eating and gum flap swelling.
If I’ve had pericoronitis before, does that make extraction more likely?
Often it does, because recurrent episodes suggest the gum flap and trapped debris are repeatedly causing inflammation. However, whether to remove the tooth depends on imaging findings, the tooth’s eruption path, and factors like complications (for example, cysts or damage to the second molar), not just one prior flare.
Is it possible for wisdom teeth symptoms to indicate an emergency?
Yes. Seek urgent care if you have fever, facial or jaw swelling that is spreading, trouble opening your mouth (trismus), difficulty swallowing, voice changes, or breathing trouble. These can indicate infection moving beyond the local gum tissue.
Does wisdom teeth eruption stop after a certain age?
Most wisdom teeth erupt between the late teens and mid-twenties, but delayed eruption into the late twenties and beyond happens. If you are in your thirties or older and develop new symptoms, it is still possible, but you should rule out other causes and get an X-ray rather than assuming it is only late eruption.
Why does my wisdom tooth feel worse after meals?
Meals can force food debris into the space around a partially erupted tooth and under the gum flap, feeding bacteria and triggering inflammation. That is why rinsing after eating and maintaining gentle, thorough oral hygiene can reduce the frequency or intensity of flares.
Next Articles

How Many Wisdom Teeth Grow: Typical Count, Timing, and Signs
How many wisdom teeth grow, typical count and eruption timing by age, plus signs, myths, and when to get X-rays

Is It Possible to Not Grow Wisdom Teeth
Learn if you can avoid wisdom teeth, what’s possible biologically, timing by age, and options like monitoring or extract

Why Do Wisdom Teeth Grow So Late? Causes and What to Do
Learn why wisdom teeth erupt late, what “late” really means, and when to seek care for impaction or delayed eruption.