That said, it has nothing to do with teeth regrowing or regenerating in the body. The ovary is not growing a new tooth the way a child grows a molar. What is happening is far more unusual, and understanding the difference matters if you or someone you care about is dealing with this finding.
The real explanation: mature teratomas and dermoid cysts
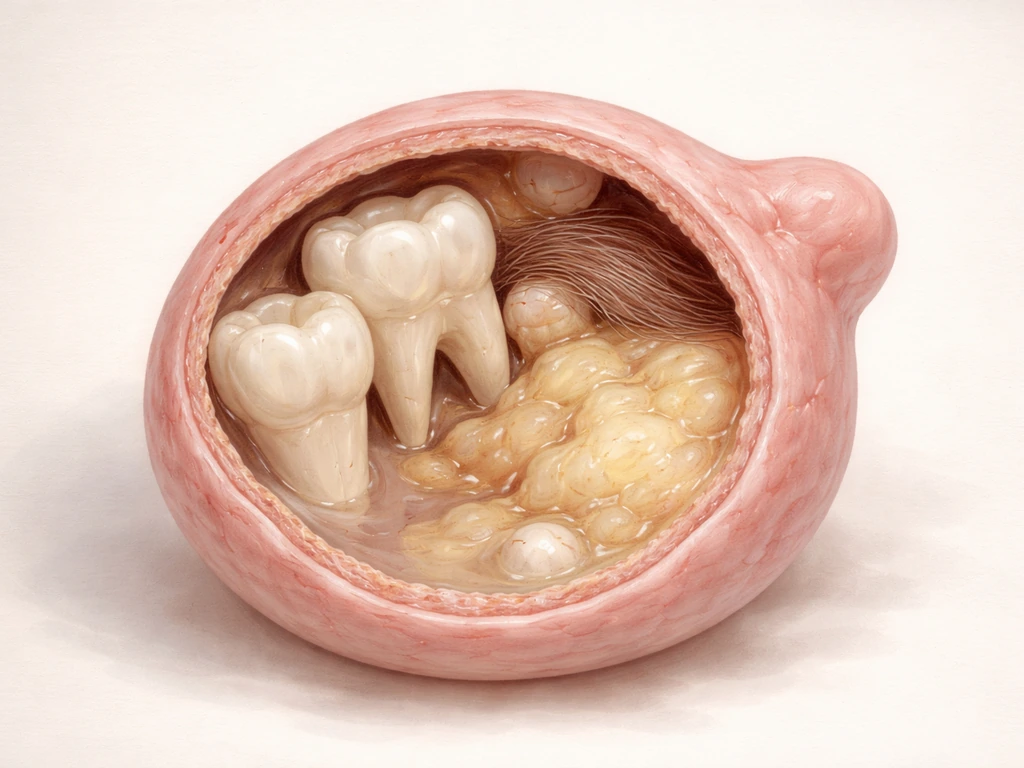
A mature cystic teratoma is the most common type of ovarian germ cell tumor. Germ cells are the cells that would normally become eggs. In rare cases, these cells go off-script during development and begin differentiating into multiple tissue types that belong in completely different parts of the body. The result is a cyst that can contain skin tissue, hair follicles, sebaceous glands, neural tissue, thyroid tissue, bone, and yes, teeth. This is not a metaphor. Pathology reports and imaging studies routinely document calcified, tooth-shaped structures within these cysts, particularly inside a dense region called the Rokitansky nodule (also called the dermoid plug), which is considered highly characteristic of a mature cystic teratoma on imaging.
The reason teeth can form here comes down to what germ cells are capable of. They carry the full genetic blueprint of the human body and, under the wrong developmental signals, can begin producing ectodermal derivatives, which is the tissue lineage responsible for skin, hair, and tooth enamel. So the tooth structures found in these cysts are not random. They are the product of the same cellular machinery that forms teeth in a developing embryo's jaw, just activated in the completely wrong location. Why teratomas grow teeth is ultimately a question of developmental biology gone wrong, not regeneration.
Teeth and hair in the same ovary: what that combination actually means

Finding both hair and teeth in an ovarian cyst is not a red flag for something more dangerous. In fact, that combination is a textbook sign of a mature (benign) teratoma rather than a malignant one. Immature or malignant germ cell tumors tend to contain poorly differentiated tissue, not the organized, well-formed structures like hair shafts and calcified teeth that you see in a mature teratoma. So counterintuitively, the more "normal" those strange tissues look under a microscope or on imaging, the more reassuring the picture is.
The hair and tooth structures form from the same ectodermal tissue lineage, which is why they appear together so often. Pathology sources consistently describe mature teratomas as containing skin, hair follicles, and teeth as a cluster of ectodermal derivatives. When a radiologist or gynecologist sees hair-density material alongside a calcified nodule on ultrasound or CT, a mature cystic teratoma jumps to the top of the differential diagnosis immediately. The pairing is that characteristic.
Normal tooth development is one of the most tightly regulated processes in the human body. It starts in the embryo and follows a precise sequence: the bud stage, cap stage, bell stage, and maturation. Each step requires exact signaling between two tissue types, the ectoderm-derived oral epithelium (which eventually produces enamel) and the neural crest-derived ectomesenchyme (which forms dentin, cementum, and the pulp). Molecular signals including BMP pathways coordinate each transition. Without this precise back-and-forth, tooth development simply stalls. This is why teeth only form in the jaw during specific developmental windows, not spontaneously in adults.
In a teratoma, those same signaling pathways get activated in the wrong place and at the wrong time because the underlying germ cells have essentially "unlocked" pluripotent developmental programs. The result can be a recognizable tooth-shaped structure with actual enamel and dentin layers, but it did not erupt through gum tissue, go through baby-tooth replacement, or follow any of the normal developmental timeline. It formed inside a cyst. This is the critical distinction between "ectopic tissue development" and actual tooth regeneration, and it is a distinction worth understanding clearly because whether stem cells can grow new teeth is a completely separate question that researchers are still working hard to answer.
How this gets diagnosed today
Symptoms that bring people in
Most mature cystic teratomas are asymptomatic and discovered incidentally, for example during a pelvic ultrasound done for an unrelated reason. When symptoms do appear, they are usually non-specific pelvic discomfort, a sensation of fullness or heaviness in the lower abdomen, or irregular periods. The more urgent presentation is acute pelvic pain, which can signal ovarian torsion. Torsion happens when the weight of the cyst causes the ovary to twist on its blood supply, and it is a surgical emergency. The typical pattern is sudden, severe one-sided pelvic pain, often with nausea, vomiting, and sometimes a low-grade fever. If that description sounds familiar, do not wait, go to an emergency department.
The imaging workup
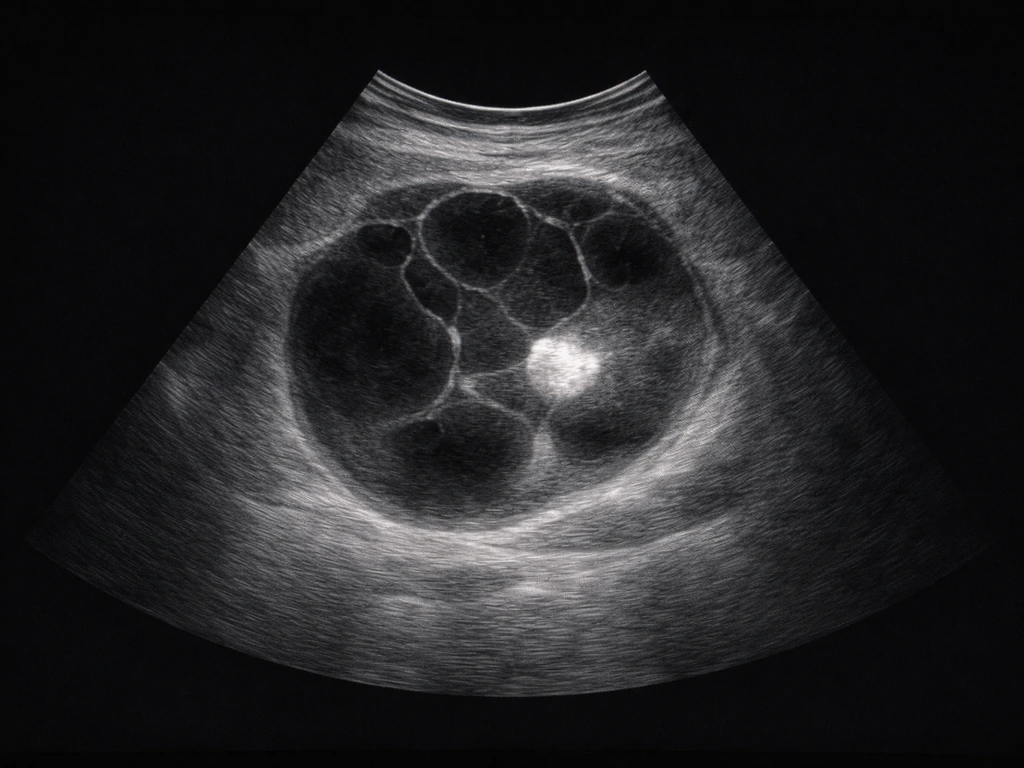
Pelvic ultrasound is almost always the first step. A mature teratoma has a very recognizable appearance: a complex cystic mass with a hyperechoic (bright) nodule, posterior acoustic shadowing from calcified structures, and often a fat-fluid level. When the ultrasound is inconclusive, CT scanning is excellent at showing tooth-like high-density structures within the Rokitansky nodule, and MRI can characterize fat content and soft tissue components even more precisely. Radiologists familiar with these findings can usually identify a mature teratoma with high confidence before any surgery. Differential diagnosis still matters though, since other ovarian masses including endometriomas, cystadenomas, and malignant tumors can look superficially similar on imaging, and cysts that grow teeth-like structures are not always benign without proper evaluation.
Lab work and tumor markers
Blood tests including AFP (alpha-fetoprotein), beta-hCG, and CA-125 are often ordered when an adnexal mass is found, particularly in younger patients or when imaging features are ambiguous. These markers help stratify malignancy risk and rule out malignant germ cell tumors like yolk sac tumor or choriocarcinoma, which look very different under the microscope but can appear as complex ovarian masses. It is important to know that tumor markers alone cannot definitively confirm or rule out malignancy. The final diagnosis always rests on pathology after surgical removal.
Treatment and what to realistically expect

For a confirmed or strongly suspected mature cystic teratoma, the standard approach is surgical removal, typically by laparoscopic cystectomy (removing the cyst while preserving the ovary) or, less commonly, oophorectomy (removing the whole ovary). The surgical choice depends on the size of the cyst, patient age, desire for future fertility, and whether the surgeon can spare healthy ovarian tissue. Indications for surgery include a persistent or enlarging adnexal mass, acute pain suggesting torsion, concern for malignancy, or a cyst large enough to pose mechanical risk.
For smaller, incidentally found cysts in patients who are not surgical candidates or who decline surgery, annual ultrasound surveillance is the accepted management approach. These cysts are typically slow-growing, which is why watchful waiting is reasonable in select cases. However, surveillance does not eliminate the risk of future complications like torsion. Surgical pathology after removal provides the definitive diagnosis, and the vast majority of these come back as benign mature cystic teratoma with no further treatment needed.
The prognosis for benign mature teratoma is excellent. Recurrence is uncommon, fertility is generally preserved when cystectomy is done carefully, and malignant transformation (which does rarely occur, usually into squamous cell carcinoma arising from the cyst lining) is estimated in less than 2% of cases, most commonly in postmenopausal women. None of this is a reason to panic, but it is a reason to follow through with the clinical workup rather than ignoring a known pelvic mass.
What teeth, enamel, and dentin can and cannot do in the body
Since this site is fundamentally about dental regeneration, it is worth being direct: the teeth found in ovarian teratomas have zero connection to the idea of regrowing lost teeth or regenerating dental tissue. They are a product of ectopic developmental biology, not regeneration. And for actual teeth, the regeneration picture is not encouraging with current biology.
Enamel, the hardest tissue in the human body, does not regenerate naturally. After a tooth erupts, the cells responsible for making enamel (ameloblasts) are gone. They do not persist in adult teeth. This means that once enamel is damaged by decay, acid erosion, or physical wear, the body has no mechanism to replace it on its own. There is currently no treatment available that can effectively regrow enamel in a clinical setting. Researchers are working on biomimetic approaches and studying whether certain cysts can regenerate dental structures, but for now, enamel loss is permanent.
Dentin is slightly more nuanced. Unlike enamel, dentin-producing cells called odontoblasts do survive in adult teeth (they line the pulp chamber), and they can produce a thin layer of reactionary or reparative dentin in response to injury. But this is a protective response, not true regeneration. It is not enough to rebuild a significant amount of lost tooth structure. And for the question of growing a whole new tooth from scratch in an adult, the honest answer right now is no. Adult tissues simply do not retain the ameloblast lineage cells needed to form enamel, which is required for a complete functional tooth. This is something researchers exploring tooth regeneration through stem cells are directly confronting.
Teratomas versus other growths: a quick comparison

| Feature | Mature Cystic Teratoma | Ovarian Cyst (Functional) | Malignant Germ Cell Tumor |
|---|
| Contains teeth or hair? | Yes, commonly | No | Rarely, and poorly formed |
| Typical patient age | Reproductive years (20s-40s) | Reproductive years | Teens to 20s |
| Tumor markers elevated? | Usually not | No | Often (AFP, hCG) |
| Imaging appearance | Fat-fluid level, calcified nodule | Simple anechoic cyst | Solid or complex mass |
| Malignant risk? | Less than 2% | Very low | By definition yes |
| Standard treatment | Laparoscopic cystectomy | Observation or OCP | Surgery plus chemotherapy |
Ovarian teratomas are not the only growths in the body capable of containing dental structures. The same ectopic tooth-forming biology shows up in other locations and contexts. If you are curious about the broader picture, it is worth knowing that tumors can grow teeth in other contexts beyond the ovary as well. Teratomas have been found in the mediastinum, retroperitoneum, sacrococcygeal region, and even the brain. The underlying biology is the same: pluripotent germ cells or residual embryonic cells activating developmental programs out of place.
There are also bony outgrowths in the jaw called mandibular tori that confuse people sometimes, since they are hard, calcified masses in the mouth that can resemble unusual dental structures on casual inspection. Understanding how mandibular tori can grow over time is a different topic entirely, but the point is that hard tissue appearing somewhere unexpected in the body usually has a specific, explainable biological mechanism, not magic or regeneration.
What to actually do if you suspect this
- If you have been told you have an ovarian cyst or adnexal mass and have not had imaging, ask your doctor for a pelvic ultrasound. This is the standard first step.
- If you have sudden, severe one-sided pelvic pain with nausea or vomiting, go to an emergency department. This could be ovarian torsion, which needs immediate surgical evaluation.
- If imaging suggests a mature teratoma, get a referral to a gynecologist or gynecologic oncologist for surgical planning and risk discussion.
- Ask about tumor markers (AFP, beta-hCG, CA-125) if they have not been checked, particularly if imaging features are not completely classic for a benign teratoma.
- If the cyst is small, asymptomatic, and imaging is reassuring, follow the recommended annual ultrasound surveillance schedule until a decision about surgery is made.
- Do not rely on symptoms alone. Many of these cysts cause no symptoms until a complication occurs, which is exactly why pelvic imaging matters when a mass is found.
The bottom line is this: ovaries can, in a very real and documented biological sense, contain teeth. But that is because of a specific developmental tumor, not because the ovary is regenerating dental tissue or doing something teeth-related on its own. The condition is usually benign, usually manageable with straightforward surgery, and very much in the domain of your OB-GYN or gynecologic oncologist, not your dentist.