The last teeth to grow in are wisdom teeth (third molars), which typically erupt somewhere between ages 17 and 25. For baby teeth, the second molars in the back are usually last, finishing up around 23 to 31 months. So whether you're tracking a toddler's teething or wondering why your back corners are still sore in your early twenties, you're in the right place.
Which Teeth Grow Last? Eruption Timing for Baby and Adult Teeth

Marcus Holloway
23 May 2026
Baby teeth: which ones are last to erupt

Most parents think teething ends after the front teeth come in, but the process actually runs well into the toddler years. Primary dentition follows a fairly predictable order: the central incisors (front teeth) usually appear first around 6 to 10 months, followed by lateral incisors, first molars, and canines. The last to show up are the primary second molars, which typically erupt around 23 to 31 months. Johns Hopkins notes that most children have their full set of 20 baby teeth by about 33 months, so the very last baby tooth to come through usually appears somewhere in that final push between 2.5 and 3 years of age.
What this means practically: if your toddler is still fussy and chewing on everything at age 2, they probably aren't done teething yet. Those back second molars are the culprit. Once those are in, primary dentition is complete and you get a break until the permanent teeth start arriving around age 6.
Permanent teeth order: which teeth are last in general
Permanent teeth follow their own multi-year sequence that mirrors the baby tooth pattern but stretched out over roughly a decade and a half. The first permanent molars and lower central incisors tend to erupt around age 6 to 7, kicking off the mixed dentition phase where kids have both baby and adult teeth at the same time. From there, the sequence moves through incisors, premolars, canines, and second molars, with the second molars typically arriving around ages 11 to 13. After that, most of the mouth is set. The notable exception, and the reason most adults have 32 teeth instead of 28, is what comes next.
| Tooth Type | Approximate Eruption Age |
|---|---|
| First molars (permanent) | 6–7 years |
| Central incisors | 6–8 years |
| Lateral incisors | 7–9 years |
| Canines (cuspids) | 9–12 years |
| First premolars | 10–12 years |
| Second premolars | 10–12 years |
| Second molars | 11–13 years |
| Third molars (wisdom teeth) | 17–25 years |
Wisdom teeth: the actual last teeth to grow in
Third molars, known as wisdom teeth, are almost universally the last permanent teeth to erupt. The Merck Manual puts their typical eruption window at 17 to 25 years, though some people see them in their late teens and others don't experience eruption until their mid-twenties. A handful of people never have them erupt at all, either because the teeth are congenitally absent (they never formed) or because they become impacted and stay trapped beneath the gumline.
Impaction is genuinely common. Research using panoramic radiographs found that roughly one in three patients showed at least one impacted tooth, and the vast majority of impaction cases involve third molars. Impaction usually happens when there simply isn't enough room at the back of the jaw for the tooth to erupt properly. The tooth can come in at an angle, press against the second molar, or break partway through the gum and stay stuck in that partially erupted state.
That partial eruption situation is worth paying attention to. When a wisdom tooth pushes through the gum but doesn't fully emerge, a flap of gum tissue can trap bacteria around the tooth, leading to a painful condition called pericoronitis. AAOMS supporting information on third molar management discusses pericoronitis and key considerations for how clinicians evaluate and manage it [leading to a painful condition called pericoronitis](https://aaoms. org/wp-content/uploads/2022/06/managementthirdmolarsupportinginformation.
pdf). If you are wondering when do teeth grow in, a wisdom tooth can often start with partial eruption before it fully emerges. Symptoms include pulsating pain around the back of the mouth, swelling, and sometimes difficulty opening the jaw fully. If you have a fever along with those symptoms, that's a sign of more significant infection and you need to see a dentist or oral surgeon promptly, not just ride it out.
What 'grow last' actually means: eruption vs. regrowth
Here's where it's worth clearing something up, because this site gets a lot of questions about whether teeth can 'grow back. ' When people search for which teeth grow last, most of them mean eruption, which is the natural process of a tooth moving through the jaw and breaking through the gum. Which teeth grow in first depends on whether you're talking about baby teeth or permanent teeth which teeth grow last.
That's a completely normal developmental event with a predictable timeline. Teething speed varies from person to person, but the timeline for eruption is usually fairly predictable. Regrowth, on the other hand, would mean regenerating a tooth that was lost or damaged, and that's an entirely different biological question with a much less optimistic answer.
Humans are diphyodonts, meaning we get exactly two sets of teeth: primary and permanent. Once your permanent teeth are in, there is no third set waiting. If a permanent tooth is knocked out, extracted, or lost to decay, the body does not replace it. Research into stem-cell-based dental regeneration is ongoing, and there are clinical approaches that can regenerate specific tissues like the pulp-dentin complex in certain scenarios, but that is a targeted clinical intervention for specific tissue damage, not a full tooth regrowing on its own. The enamel on existing teeth also cannot regenerate once it's gone, which is why enamel loss leads to sensitivity and why protecting it matters.
So if you're wondering which teeth 'grow last' because you're hoping a lost adult tooth might still come in, the answer is no. But if you're tracking whether wisdom teeth or other late-erupting teeth haven't shown up yet, that's a normal developmental question worth monitoring. If you're asking how long for front tooth to grow in, the timeline depends on whether you're talking about baby central incisors or permanent front teeth.
When to actually worry: delayed eruption, impaction, and spacing

Not every late-erupting tooth is a problem. There's a wide range of normal. But there are situations where a delay signals something that needs professional attention.
- A child has no baby teeth by 12 to 15 months (may warrant checking in with a pediatric dentist)
- Primary second molars haven't appeared by age 3 to 3.5 years
- A permanent tooth is expected but hasn't erupted years after its typical window (for example, still no canines by age 14)
- A permanent tooth erupted on one side but not the other (asymmetric eruption is often a red flag)
- A baby tooth was lost very early due to decay or injury and no permanent tooth has followed
- Visible swelling, pain, or pus at the back of the mouth where a wisdom tooth should be coming in
- Crowding, shifting, or bite changes in the back of the mouth
Primary failure of eruption is a real (if uncommon) condition where teeth simply don't move into the mouth as expected, and it can have both local causes (like a physical obstruction or ectopic position) and systemic ones. If a tooth has been expected for more than a year past its normal window and hasn't appeared, that's worth imaging, not just watching.
How to confirm what's happening: X-rays and the right appointments
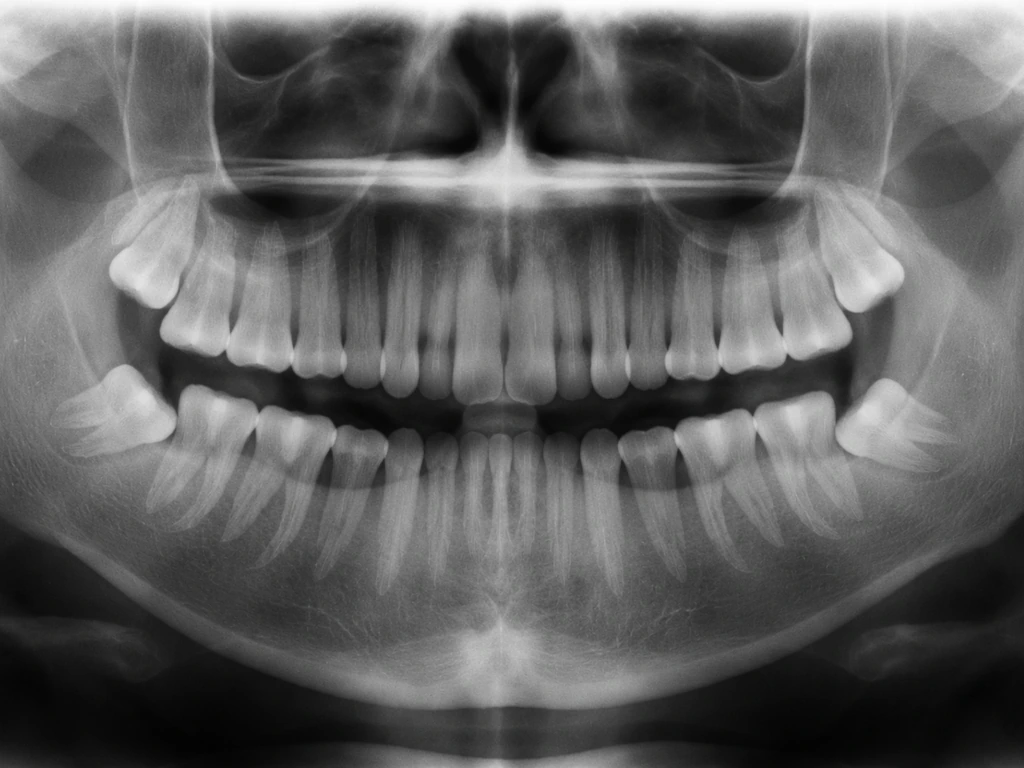
The best tool for understanding what's going on with late or missing teeth is a panoramic X-ray (also called an OPG or panorex). This single image captures all your teeth, including unerupted ones still sitting in the jaw, their angles, and how much room they have. It's routine for orthodontic assessments and for evaluating wisdom teeth. A dentist or orthodontist can look at a panorex and tell you immediately whether a tooth is present but unerupted, developing normally, impacted, angulated incorrectly, or absent entirely.
The American Association of Orthodontists recommends that children get an orthodontic screening by age 7. That may sound early, but it's exactly the right time to spot problems with incoming permanent teeth, spacing issues, and early signs of impaction before they become harder to treat. You don't need to be in braces or have obvious problems to get this screening. Most orthodontists offer an initial evaluation at no charge.
For adults concerned about wisdom teeth, the conversation is usually with a general dentist first. They'll take a panoramic X-ray (or refer you for one) and can assess whether wisdom teeth are erupting, impacted, or absent. If surgical removal is needed, they'll typically refer you to an oral and maxillofacial surgeon. CBCT (cone beam CT) imaging provides even more detailed 3D information about angulation and root proximity to nerves, which is sometimes ordered before wisdom tooth extraction.
Next steps if teeth aren't erupting normally
For parents of toddlers or kids
If your child is in the expected window but still behind on teething, keep their regular well-child dental visits (most guidelines recommend a first dental visit by age 1). Ask the dentist to confirm that all primary teeth are present and developing correctly. If a tooth is significantly late, ask specifically whether imaging is appropriate. For teething discomfort, chilled (not frozen) teething rings and gentle gum massage are safe options. Avoid teething gels containing benzocaine in young children.
For teens and young adults waiting on wisdom teeth
If you're in your late teens and your wisdom teeth haven't erupted yet, that's completely normal. Most dentists begin monitoring third molars with panoramic X-rays in the mid-teen years to track development and position. AAPD radiograph prescribing guidelines recommend selecting imaging types based on developmental stage, including monitoring third molars using appropriate panoramic exams in adolescents before third molars erupt [panoramic X-rays](https://www. aapd.
org/assets/1/7/E_Radiographs1. PDF). You don't need to do anything until a dentist recommends it, but you should be keeping regular dental appointments so the situation gets watched. If you're already feeling pressure, soreness, or swelling at the very back of your mouth, get evaluated sooner rather than later.
Partially erupted wisdom teeth that are symptomatic often benefit from extraction before the situation escalates.
Managing discomfort while waiting
While waiting for late-erupting wisdom teeth or other slow-arriving permanent teeth, over-the-counter ibuprofen or acetaminophen can manage soreness. For wisdom tooth gum inflammation specifically, rinsing with warm salt water a few times a day can reduce bacterial load around a partially erupted tooth and ease minor inflammation. Keep the area as clean as possible with careful brushing and flossing. If pain increases, swelling spreads toward your cheek or throat, or you develop a fever, skip the home remedies and call a dentist or oral surgeon that day. Those are signs of infection that need professional treatment, not just pain management.
The bottom line: wisdom teeth are the last teeth to grow in for almost everyone, and their eruption timeline runs well into adulthood. Whether you're tracking a toddler's final baby teeth or your own long-awaited third molars, understanding the normal sequence helps you know when to be patient and when to make an appointment. For adults concerned about wisdom teeth, the conversation is usually with a general dentist first toddler's final baby teeth. A panoramic X-ray and a conversation with your dentist is always the clearest path to knowing exactly where things stand.
FAQ
If my wisdom teeth are the last teeth to grow in, what age should I expect them to start showing on X-ray or in the mouth?
Even when eruption is delayed, third molars usually start developing years earlier. Dentists often use panoramic X-rays in the mid-teen years to confirm the tooth is present, how it is angled, and how much space exists, so the “start” can mean tooth development on imaging even before you see it break through the gum.
Is it normal for only one wisdom tooth to come in while the others do not?
Yes, it can be normal. Asymmetry is common because each third molar’s angulation and available space differ. One side may erupt partially or fully while the other stays impacted or never erupts.
What counts as “too late” for a tooth that’s supposed to erupt, and when should I stop waiting?
A practical rule is to consider evaluation if a tooth is more than about a year past its typical eruption window, especially for permanent teeth. At that point, ask about an X-ray (often a panoramic) to determine whether the tooth is present but delayed, angled, or missing.
If my child is not done teething by age 2, could something be wrong besides normal variation?
Most of the time it’s normal, particularly if the primary second molars are still missing. However, if you also see unusual swelling, trouble feeding, or if you suspect a specific tooth has been absent beyond the expected range, request a dental exam and ask whether imaging is appropriate.
Can a wisdom tooth grow in sideways or at an angle and still erupt normally?
Sometimes it can erupt partially, but an angled third molar is more likely to cause crowding, press on the second molar, or get stuck. That’s why dentists assess both position and space on a panoramic X-ray, and they may use CBCT in complex cases.
What’s the difference between a wisdom tooth “partially erupted” and a tooth that’s impacted?
Partially erupted means the crown has started breaking through the gum, but the tooth is not fully emerged. Impacted means it remains trapped within the jaw, often covered by gum and sometimes angled toward another tooth.
If I have symptoms around a partially erupted wisdom tooth, do I need antibiotics right away?
Not automatically. Many cases start as inflammation (pericoronitis) and can improve with evaluation, oral rinses, and pain control. Antibiotics are more likely when there are clear signs of spreading infection, such as fever, rapidly worsening swelling, or difficulty swallowing.
Can late-erupting permanent teeth mean my child will need orthodontics later?
Not necessarily, but late or slow eruption can sometimes reflect spacing issues or abnormal tooth positioning. A key decision point is whether the panoramic X-ray shows adequate space for the tooth to come in; if not, orthodontic screening can help prevent more complicated problems.
Why does a panoramic X-ray help more than a regular exam when teeth seem delayed?
A panorex shows unerupted teeth and their angles, not just what’s visible in the mouth. That lets a dentist determine whether a tooth is present but trapped, coming in from an unusual direction, or absent due to developmental variation.
Are there common reasons “regrowth” of a lost adult tooth is expected in searches, and what is actually possible?
A lost adult tooth usually will not regrow because humans are diphyodonts, meaning there is no third set of replacement teeth. Regenerative dentistry is limited to specific tissue repair scenarios, but it is not the same as a whole new tooth growing back.
Next Articles

Which Teeth Grow in First? Baby Tooth Eruption Order
Baby tooth eruption order: which teeth come first, timing range, normal teething signs, and when to see a dentist.

How Fast Do Teeth Grow Timelines for Eruption and Development
Timelines for tooth eruption and true dental growth, plus what affects speed, normal vs abnormal, and no enamel regrowth

When Do Teeth Grow In? Eruption Timeline by Age
Tooth eruption by age: when baby and permanent teeth arrive, wisdom teeth timing, and when delays mean you should see a